Over the past decade, many changes and updates have occurred in the world of vascular anomalies, including their histopathology. An appreciation has developed that a combined team approach is optimal in arriving at a correct diagnosis. Technical advances such as immunohistochemical stains for GLUT1, an excellent marker for infantile hemangioma, and vascular immunostains such as D2-40, PROX1, and vascular endothelial growth factor receptor 3, which distinguish lymphatics from arteries and veins, have been of immense help in daily practice.
Over the past decade, many changes and updates have occurred in the world of vascular anomalies, including their histopathology. A significant step was the adoption of the Mulliken and Glowacki proposal of dividing vascular anomalies into tumors and malformations by the International Society for the Study of Vascular Anomalies in 1996. This classification system allowed more meaningful communication between colleagues, helping to eliminate diagnostic and therapeutic errors. Emergence of vascular anomalies centers has facilitated identification of new vascular anomalies and their underlying genetic causes. An appreciation has developed that a combined team approach is optimal in arriving at a correct diagnosis, or at least at an appropriate working diagnosis when uncertainty exists. Furthermore, technical advances such as immunohistochemical stains for GLUT1, an excellent marker for infantile hemangioma, and vascular immunostains such as D2-40, PROX1, and vascular endothelial growth factor receptor 3 (VEGFR-3), which distinguish lymphatics from arteries and veins, have been of immense help in daily practice.
Vascular tumors
Infantile Hemangioma
The proliferative phase of cutaneous infantile hemangioma shows a dermal/subcutaneous lesion composed of lobules and sheets of tightly packed, mostly capillary-sized vascular channels ( Fig. 1 A). The endothelial cells are plump and the basement membranes are thin and surrounded by a layer of pericytes (see Fig. 1 B). The minimal intervascular stroma contains predominantly a few fibroblasts and mononuclear cells, including mast cells. Mitoses are observed. The involutive phase is characterized by diminution in the number of channels, luminal enlargement, flattening of endothelium, waning mitotic activity, apoptotic figures, and thickening of basement membranes (see Fig. 1 C). The fibrous stroma between channels is increased, mast cells remain, and the arteries and veins in the interlobular stroma appear relatively prominent. In the involuted phase, the fibrofatty background is dominant, the dermis often shows scarring with loss of elastic fibers and absent appendages, and the skin surface is wrinkled. Residual capillaries are sparse, single, or clustered. They are often tiny and “ghost-like” with thick, hyalinized basement membranes, and occluded lumens containing apoptotic debris (see Fig. 1 D). The large feeding and draining vessels with intimal fibrosis may still be present.
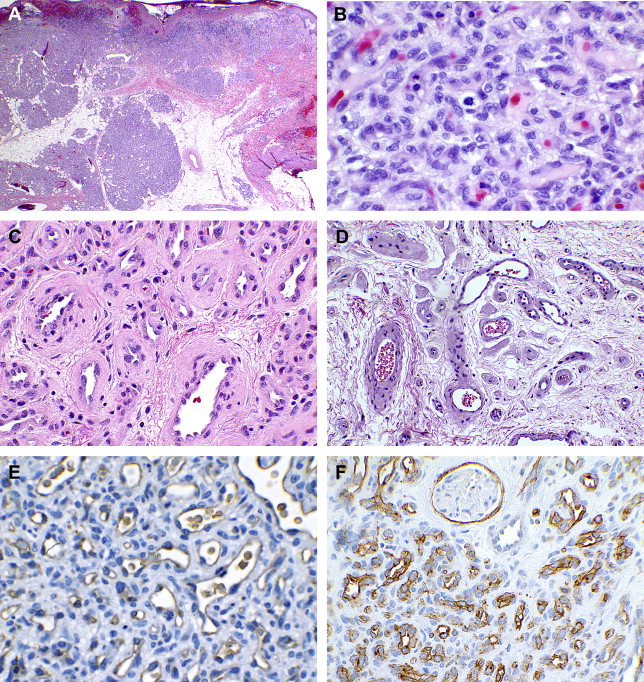
The most useful immunohistochemical marker for diagnosing infantile hemangioma is glucose transporter protein isoform 1 (GLUT1). It is a cytoplasmic endothelial stain expressed in infantile hemangioma at all stages of evolution (see Fig. 1 E, F). Antibodies to CD31 (panendothelial cell marker) and CD34 (vascular endothelial marker) also stain the endothelial cells but are not specific for infantile hemangioma. Smooth muscle actin (SMA) highlights pericytes and vascular smooth muscle. KI-67, a proliferative index marker, may be 20% or greater in the endothelial cells and pericytes in the proliferative phase.
Congenital Hemangiomas
Congenital or fetal hemangiomas differ from infantile hemangiomas in that they are fully developed at birth with little to no growth postpartum. There are two types of congenital hemangiomas, rapidly involuting congenital hemangiomas (RICH) and noninvoluting congenital hemangiomas (NICH).
Rapidly involuting congenital hemangioma
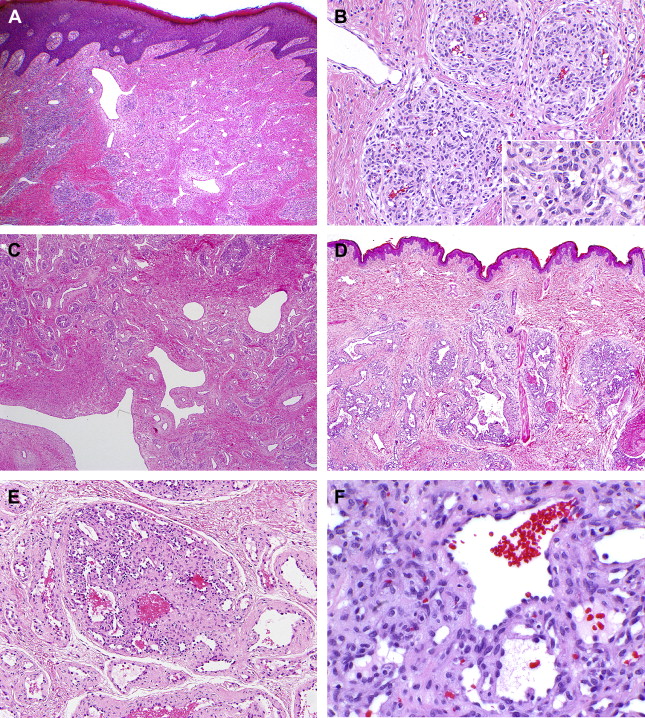
RICH is a circumscribed, raised lesion with a central depression, scar, or ulceration surrounded by a rim of pallor. Histology shows dermal and subcutaneous lobules of capillaries, occasionally coalescent, surrounded by abundant fibrous tissue ( Fig. 2 A). The lobular capillaries have moderately plump endothelium and a thin basement membrane surrounded by a layer of pericytes (see Fig. 2 B). The center of many RICHs shows advanced involution with absence of lobules, abundant fibrous tissue, and residual draining veins, many being large and abnormal with thickened and irregular fibromuscular walls (see Fig. 2 C). The endothelial cells are immunonegative for GLUT1, although rarely a few cells may be positive. Extramedullary hematopoiesis, arteriovenous shunts, aneurysms, cysts, hemosiderin, and thrombi may be present.
Noninvoluting congenital hemangioma
NICH generally resembles RICH in its external appearance. Minor differences in the former include greater elevation and coarse telangiectases. When NICH is removed at several years of age, histopathology shows lobules that are variable in size and most often large (see Fig. 2 D) and composed of curved, thin-walled capillaries. The endothelial cells have minimal cytoplasm and small, hyperchromatic nuclei that protrude into the lumen (see Fig. 2 E, F), and frequently contain cytoplasmic eosinophilic globules. The centrilobular vessels tend to be larger and surrounded by fibrous tissue. Endothelial cells are immunonegative for GLUT1. Interlobular fibrous tissue is abundant and contains prominent arteries and veins, and arteriolobular fistulae may be present. Some lesions have diminished or even few lobules, and are composed primarily of arteries, veins, and fibrous tissue, thereby mimicking a vascular malformation. The histopathologic appearance of NICH removed at an early age, such as 2 years, is similar to RICH without the central zone of advanced involution. NICH, excised in adolescence, tends to have few lobules with the major part of the lesion consisting of prominent interlobular arteries and veins.
Other Vascular Tumors
Tufted angioma
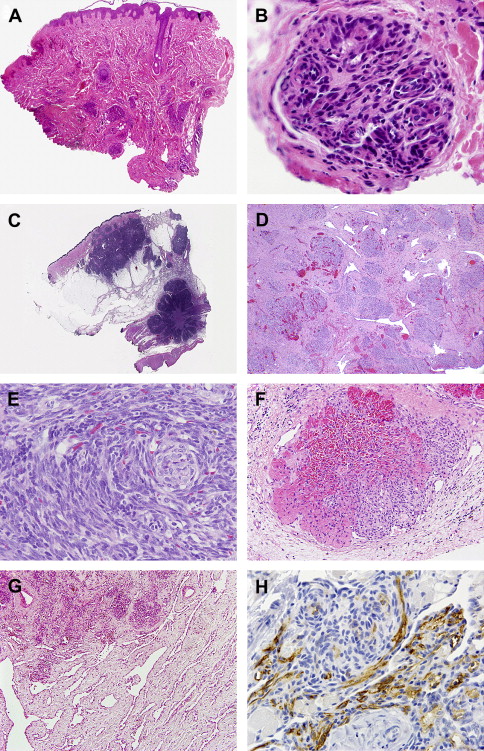
Tufted angioma (TA) typically presents as enlarging pink–red macules and plaques in the upper chest, back, and neck in young children. Histopathology shows lobules dispersed in the dermis and subcutaneous tissue, often referred as cannonball , because of their frequent rounded shape ( Fig. 3 A). The lobules themselves may be somewhat compartmentalized into miniature lobules. They are composed of capillaries with slightly plump and sometimes spindled endothelial and perithelial cells (see Fig. 3 B). Focally, the spindled cells are highlighted by the D240 and PROX-1 immunoreaction. Thin-walled draining channels partially surround the lobules.
Some lesions that look like TA clinically have a histopathologic appearance suggestive of, or even indistinguishable from, kaposiform hemangioendothelioma (KHE) with coalescent lobules, microthrombi, hemosiderin deposits, and reactive stroma. Generally, a firm histopathologic diagnosis of TA is not advisable and appropriate therapy will depend on clinical evolution of the lesion. Conversely, selected microscopic fields in KHE may be similar to those seen in TA. Generally, a firm histopathologic diagnosis of TA is not advisable and appropriate therapy will depend on clinical evolution of the lesion. Many observers believe that there is clinical and histopathologic overlap between TA and KHE, with TA being at the less aggressive part of the spectrum.
Kaposiform hemangioendotheliomas
KHE are locally aggressive tumors that occur in many locations, particularly skin, subcutis, deep soft tissue, retroperitoneum, mediastinum, and rarely bone. Half are congenital and most are present before the age of 2 years. KHEs are grossly, ill-defined vascular stains, plaques, or deep-seated bulging lesions. Vascular tumors larger than 5 cm are often associated with marked thrombocytopenia (Kassabach-Merritt phenomenon). KHEs histopathologically are infiltrative lesions usually involving multiple tissue planes characterized by coalescing and poorly canalized lobules composed of rounded or spindled endothelial cells and pericytes (see Fig. 3 C, D). The degree of spindling varies among lesions, as do clusters of rounded cells, focally imparting a glomeruloid appearance (see Fig. 3 E). Nuclei may focally be very small and dense. Nuclear atypia is absent and mitoses are rare. Thrombi or platelet aggregates within the lobular capillaries are almost always identified and the lesional cells often contain hemosiderin. Some KHEs have foci of larger channels containing closely packed erythrocytes, and in some tumors this is a dominant feature (see Fig. 3 F). Thin-walled channels often surround the lobules (see Fig. 3 D). The lesional cells are immunoreactive for CD31, and the spindled cells focally for D2-40 (see Fig. 3 F) and PROX-1. Ki-67 typically shows a low proliferative index. The perilobular stroma shows varying combinations of edema, myxoid change, and fibrosis. Many KHEs have vicinal dilated lymphatic channels (see Fig. 3 G), and occasionally lesional cells seem to proliferate within them. KHE is negative for HHV-8 by immunostain and reverse transcription–polymerase chain reaction, implying a pathogenesis different from that of Kaposi sarcoma.
Pyogenic granuloma
Pyogenic granuloma (PG), also known as lobular capillary hemangioma , is a common acquired lesion of the skin and mucous membranes, most often in the head and neck region. They are commonly seen in pregnant women and children and are associated with a history of trauma, hormonal alterations, and medications. PGs can arise within a capillary malformation. Congenital solitary and congenital disseminated PGs have also been reported.
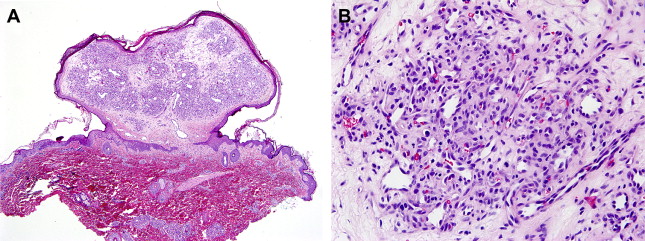
PG is a polypoid dermal lesion composed of lobules of curved capillaries and venules lined by plump endothelial cells ( Fig. 4 A). The individual capillaries and lobules are separated by edematous to fibrotic stroma with scattered inflammatory cells (see Fig. 4 B). The overlying epithelium may be atrophic and ulcerated and frequently shows lateral collarettes or indented hyperplastic surface epithelium encasing the lesion (see Fig. 4 A). A prominent feeding artery is often seen at the base of the lesion. If ulceration ensues, a rind of inflammatory granulation tissue may overlie the lesion. In the late stages, a decreased number of lobules is present and the stroma is more fibrotic. Some lesions are deep-seated and involve the reticular dermis or subcutaneous tissue only, and rarely PG may occur intravascularly. In the absence of epidermal changes, PGs may superficially resemble an infantile hemangioma, but the curved channels, intervascular stroma, and epidermal collarettes in PG are helpful distinguishing features, as is the patient’s age. If uncertainty exists, the GLUT1 immunostain will differentiate the two because PGs are negative.
Vascular malformations
During embryogenesis, normal blood vessels are derived from two processes: vasculogenesis (the process through which endothelial precursors align themselves to form primitive blood vessels) and angiogenesis (development of new vessels). Experts speculate that an error in both or either one of these processes results in malformed vessels. Vascular malformations occur in less than 1% of the population.
Capillary Malformation
The term capillary malformation (CM) is used in a generic sense by clinical colleagues to indicate a vascular stain of the skin rather than a specific type of lesion. Therefore, CM includes stains produced by various vascular malformations, such as the common facial “port-wine” stain (venocapillary malformation), lymphaticovenous malformations, venous and arteriovenous malformations, and those observed in syndromes such as Klippel-Trénaunay and Parkes Weber.
The most common and well-known CM is the facial nevus flammeus or “port-wine” stain. Biopsies of lesions in young children may show only rare dilated “capillaries” in the papillary dermis. With increasing age, CM is characterized by haphazardly arranged ectatic vessels, with small venular morphology in the papillary and occasionally reticular dermis. The channels have flat endothelial cells, thin collagenous walls, and a layer of pericytes (see Fig. 5 A). Vascular size and the mean vessel area increase with age and correlate with the change in color of the lesion.
Related posts:
 Vascular Anomalies: Current Overview of the Field
Vascular Anomalies: Current Overview of the Field
 Pathogenesis of Vascular Anomalies
Management of Venous Malformations
Pathogenesis of Vascular Anomalies
Management of Venous Malformations
 Management of Arteriovenous Malformations
Management of Arteriovenous Malformations
 Management of Combined Vascular Malformations
Management of Combined Vascular Malformations
 Special Considerations in Vascular Anomalies: Operative Management of Craniofacial Osseous Lesions
Special Considerations in Vascular Anomalies: Operative Management of Craniofacial Osseous Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


