The success of the Mohs procedure depends on the reliability of each step in the technique. Pitfalls in histologic preparation of the tissue specimens may occur during debulking, excising, orienting, creating the map, sectioning, inking, tissue flattening and freezing, cutting, slide fixation, staining, and mapping the tumor. Challenges are also present in interpreting the slides. Diagnostic pitfalls include floaters, inflammatory conditions resembling tumor, and perineural invasion. The technique requires time, teaching, and a sufficient quantity of cases from which to learn, as well as attention to the pitfalls that occur while processing tissue specimens and interpreting and mapping the histology.
The Mohs micrographic surgical procedure is an important modality that achieves the highest cure rate for most common skin cancers using an intraoperative stepwise histologic evaluation of surgical margins. The success of the procedure is inherently tied to the reliability of each of many steps that make up the technique. Pitfalls in histologic preparation of the tissue specimens may occur during debulking, excising, orienting, creating the map, sectioning, inking, tissue flattening and freezing, cutting, slide fixation, staining, and mapping the tumor. Challenges are also present in the interpretation of the slides. This article discusses some of the histologic pitfalls of the Mohs technique.
Technical pitfalls
Because Mohs surgery involves many steps between taking the tissue from the patient and having the slides ready for interpretation, there are many chances for human error and technical problems ( Table 1 ).
| Potential Pitfall | Recommendation | |
|---|---|---|
| Debulking | Curettage may create jagged borders, epidermal loss, or induce floater | Curettage when indicated instead of routinely doing it, saline irrigation after excision |
| Excising | Cutting into cancerous tissue if bevel angle <15°; thick and tall edges if bevel angle >45° Cutting marginal surfaces when making relaxing incisions | Bevel angle of 30° to 45°, use relaxing incisions when tissue doesn’t lie flat Make the relaxing incisions close to the center of the specimen |
| Orienting | Tissue rotation Introducing floaters when making the hash marks | Double-hash at one point, asymmetric hash marks, saline irrigation |
| Mapping | Inaccurate mapping | Consistency regardless of the mapping method |
| Sectioning | Inducing tissue lacerations which may be mistaken for hash marks | Controversial whether Mohs surgeon or histotechnician should do the sections. Number of tissue sections are a matter of debate as well |
| Inking | Placing it in the wrong margin, inadequate inking, ink running over the wrong sections | Controversial whether Mohs surgeon or histotechnician should do the inking. High-quality ink, appropriate amount of ink |
| Tissue Flattening and Freezing | Ice crystal formation if frozen too slowly leading to cracks and holes in the specimen; curling the tissue if blades are not cold enough | Appropriate temperature from −22°C to −30°C. Cold cutting blades |
| Cutting | Tearing or curling the tissue with dull blades; tear in the tissue if nicks on the blade; thick specimen with loose screws; inducing floaters | Use sharp blades; check blades for nicks; try to achieve the thinnest sections possible; check the screws; clean the blades |
| Slide Fixation | Artifact due to short time dehydration; tissue doesn’t attach due to defects on the slides; errors in labeling | Appropriate dehydration time; check for defects on the slide; proper labeling |
| Staining | Artifacts if not long enough time for dehydration; floaters if staining solution is contaminated | Complete dehydration, change staining solution frequently |
Debulking
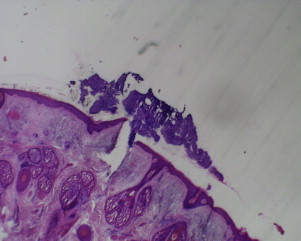
Mohs surgeons typically use curettage for tumor debulking to remove friable tumor-infiltrated dermis, thereby more accurately defining the tumor margins. Whether preoperative curettage can offer a more precise first-stage excision without compromising tissue conservation remains a subject of debate. Some researchers argue that preoperative curettage may remove normal, healing, and/or actinically damaged skin, creating an unnecessary larger wound that subsequently requires fewer Mohs stages for tumor clearance. In contrast, some researchers have shown that preoperative curettage may be tumor-specific and potentially assists in delineating the subclinical extensions of the tumors. Because there is no evidence-based recommendation regarding preoperative curettage, at present, the decision to perform preoperative curettage rests largely on an individual surgeon’s preferences and personal experience. Mohs surgeons should be aware of several pitfalls encountered during pre-Mohs curettage. The curette may not remove tissue in a uniform fashion with smooth sharply defined borders. If curettage yields jagged edges, it is difficult to take a uniformly narrow specimen during Mohs’ surgery. In addition, curettage can create shearing forces in the surrounding epidermis, which may lead to epidermal loss during tissue processing. Curetting severely photodamaged skin in areas such as the forearm and cheek may sometimes create overhanging pieces of epidermis at the edges. Furthermore, preoperative curettage may increase the incidence of floaters ( Fig. 1 ).
Excising
To achieve a flat pancakelike Mohs layer the optimum bevel angle is from 30° to 45°. A bevel angle less than 15° increases the chance of cutting into the cancerous skin thereby increasing the number of Mohs layers and the diameter of the defect. On the other hand, a bevel angle greater than 45° interferes with proper tissue flattening for optimal sectioning. Specimens that are cut thickly or with tall 90° edges do not lie flat on their own. In such circumstances, there is a higher chance of losing epidermal and/or dermal margins. It is therefore necessary to make relaxing incisions to improve tissue flattening. A potential pitfall is to cut the marginal surface while making the relaxing incisions, which can confuse the orientation as well as interrupt the continuity of the margin. Pitfalls can also occur when taking additional layers for second and subsequent Mohs stages. These sections can be rectangular or crescent shaped. Some investigators think that when a rectangular specimen is taken, tumor may hide in the part of the margin at the end, distal to the acute margin. To avoid a false-negative view, relaxing cuts need to be made in a way such that the 90° angle of the vertical edges is converted to a curved line. This cut can be difficult to perform, especially in narrow specimens. Therefore, some investigators suggest using crescent-shaped sections instead of rectangular sections.
Orienting
The surgeon has many ways of marking the tissue for orientation. Most surgeons create hash marks (nicks) cutting into both the specimen and the edge of the wound simultaneously. Frequently, a nick is created at the 6- and 12-o’clock (or 3- and 9-o’clock) positions in anticipation of a bisected specimen. A potential pitfall for this method is that the tissue may be rotated from the time it is excised to the time it gets to the laboratory. To avoid this rotation, some Mohs surgeons make asymmetric nicks (eg, at the 3- and 12-o’clock positions) or a double nick at 1 point (eg, at the 12-o’clock position). Asymmetric nicks can, however, lead to distortion on the maps in bisected specimens because the bisected line is the result of estimating the half of the specimen. Regardless of the method used by the surgeon, consistency of the orienting method helps to minimize the errors because it provides the ability to the surgeon, the histotechnician, and all the assistants to predict and then identify the right orientation of the tissue without difficulty. Another pitfall that Mohs surgeons should be aware of is that when the tissue is scored from the surface to the depth, a floater can be introduced by forcing tissue at the surface down to the base, producing a false-positive margin (see Fig. 1 ).
Creating the Map
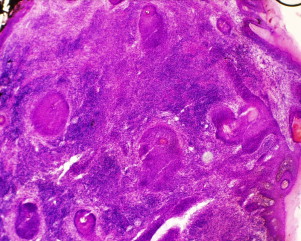
Inaccurate mapping results in false-negative subsequent layers and failure of the technique and may account for some tumor recurrences. There is variability in mapping methods used by Mohs surgeons. Silapunt and colleagues showed in a survey that most of the Mohs surgeons prepare tissue maps themselves using hand-drawn pictures to map and orient specimens. This method is fast and inexpensive. Hand-drawn pictures, however, cannot provide the exact size and shape of the excised area; therefore, these investigators suggest the use of digital and Polaroid photographs, which can produce detailed representations of defects, the excised tissue, and their interrelationship ( Fig. 2 ). There are other methods for mapping, such as using preprinted maps or cartoons of anatomic sites. There is no study to show which mapping method is superior in preventing errors. However, consistency of mapping by whichever method used allows for predictability and thus better accuracy.

Sectioning
Many Mohs surgeons cut the tissue into 2 pieces in the first stage. However, the first-stage tissue may be divided into 3 or 4 pieces in certain circumstances. Cutting into more pieces is more expensive and time consuming but may provide better sections for evaluating epidermal margins. However, there is a higher chance of mislabeling or mixing up the specimens or mismapping positive margins when there are more pieces. Another problem with multiple small sections is the higher likelihood of folding at the epidermal edges, which may lead to false-positive results. In addition, the technician may assume tissue lacerations as hash marks and may make incorrect sections. Hence, some Mohs surgeons section the specimen in the procedure room to reduce the chance of incorrect cuts and inaccurate mapping. However, other surgeons consider that sectioning and grossing by the histotechnician under magnified light allows for better tissue preparation. Still other surgeons prefer that the first stage be processed as 1 piece (pac-man technique), so that orientation cannot be misconstrued. This option works only for relatively small pieces and requires exceptional skill on the part of the person using the cryotome to section the tissue.
Inking
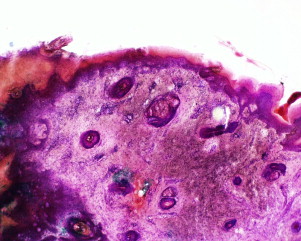
Inking can be done by the surgeon in the procedure room or by the histotechnician. Some Mohs surgeons prefer to do the inking in the procedure room to reduce the chance of placing ink on the wrong margins. This procedure can, however, be more time consuming for the surgeon, as well as increase the expense because it requires multiple magnifiers and inking equipment in each room. Furthermore, the surgeon should be well acquainted with sectioning because after inking he/she cannot further cut the tissue if the specimen is too large. Inking is most helpful when the ink is placed along a significant portion of the surgical margin rather than just as an orienting dot at the specimen pole ( Fig. 3 ). If the specimen is inked along the entire margin, missing ink indicates that a margin is not fully evaluable. On the other hand, if too much ink is used, ink may inadvertently run over and confuse the margins. The same problem can also occur if the specimen is too wet. Quality of the ink is important too. Poor-quality ink may be washed off during the tissue preparation.

Tissue Flattening and Freezing
This step is critical for achieving sections in which it is possible to examine the complete en face outer margin of a specimen. Proper flattening makes it possible to section the complete undersurface, the sidewall, and the epidermal margin in a single piece. Several methods are used for flattening: heat-extractor flattening with optimal cutting temperature (OCT) medium in the cryostat, tissue cuts or slits, aerosol freezing on a glass slide, mechanical flattening with liquid nitrogen, or different combinations of these methods. Flattening the tissue can be challenging when the edges are vertical, requiring relaxing cuts to be made. If there is inadequate relaxation of the tissue, peripheral margins may not be teased down, which results in missing epidermis. In some anatomic areas such as periocular tissue, flattening and embedding can be difficult, because delicate periocular tissue may fold easily before embedding.
The tissue should be kept adequately frozen, at −22° to −30°C, to obtain good-quality frozen sections. Colder temperatures of −28° to −32°C may be required for fat-containing tissue. If tissue is frozen too slowly, ice crystals can leave holes in the tissue. Condensate that accumulates in humid conditions can also result in ice crystal formation that causes cracks and holes in the specimen. If the cutting blade in the cryostat is not cold enough, either the sections tend to attach to the blade or the tissue may curl during the cutting. High humidity in the room can also lead to curling of the specimen.
Cutting
Blades are either permanent or disposable. Dull blades may cause tearing or curling of the tissue, or sometimes cause chatter lines in the tissue as they cut. It is therefore important to sharpen the permanent blades and to move the disposable blades along the blade holder over the course of the day. It is also important to check the blade for nicks. A small microscopic nick in the edge of the blade can create a large tear in the tissue.
The goal in cutting is to achieve the thinnest sections possible because this promotes ease in having the entire epidermis visible on the slide. However, it is difficult to obtain sections thinner than 3 to 4 μm. Thick sections are also difficult to read because some of the cellular details may be obscured ( Fig. 4 ). If the knife or chuck screws are loose, the sections may be cut thin in one section and thick in another. Thin sections may make it difficult to cut fat, and holes or tears may be visible. For this reason, thicker sections may be cut. Because the evaluation of both fat and epidermis/dermis is important, alternating thicker and thinner sections may be optimal. Another potential pitfall during cutting is the introduction of a floater from the blade. In this case, the fragment may be visualized on multiple cuts on the slide and may be directly continuous with the true specimen (in contrast to the floaters from the contaminated staining well; see later discussion). The Mohs histotechnician can minimize the potential for introducing floaters by ensuring that the cutting surface and cryostat blade are cleaned between the cases and that the staining solutions are changed frequently. Challenges also occur when the section is slid from the blade onto the slide. After placing each section on the slide, the extra OCT medium around it should be wiped off the glass slide before placing the subsequent specimen. If the subsequent section is placed over the OCT medium, it may not adhere properly during the fixation and as a result it can be washed off the slide during staining. The space between the specimens on the glass slide should be wide enough to avoid overlapping OCT medium with the tissue sections. In addition, if the OCT medium covers the tissue, it may interfere with proper tissue staining.
Slide Fixation
Slide fixation involves the use of chemicals or heat to adhere the tissue to the slide before staining. Mohs laboratories typically use 10% neutral buffered formalin, alcoholic formalin, alcohol, or acetone as a fixative for frozen section slides before staining. Alcohol seems to be the most popular choice, especially because the other 3 agents require the use of a hood. If the slides are removed too quickly from the fixative, they will not have enough time for dehydration, which affects the staining quality (see Fig. 3 ). Another potential pitfall in the slide fixation process is a flaw with the glass slide. If glass slides have any defects or are dirty, tissue may not adhere properly to them. Slides can have frosted or unfrosted ends. The frosted end in slides is usually used to identify the first section that is cut. So slides with a frosted end are preferred because they decrease the chance of confusing the sections. Proper labeling is of utmost importance. Typically, slide labels should include the patient’s last name, stage of the surgery, section and level cut, date, and the histotechnician’s initials.
Staining
Most Mohs surgeons use hematoxylin-eosin (H&E) for staining. Maintaining quality with H&E staining can be difficult. The staining steps are postfixation preparation, nuclear staining, cytoplasm staining, dehydration, clearing, and cover slipping. Of note, stains are particularly subject to pH changes. Dehydration is also very important to the final outcome. Unless all water is removed, the final slides will have artifact and be difficult to read ( Fig. 5 ). Some Mohs surgeons prefer toluidine blue staining. Toluidine blue stains the mucin bright red and, therefore, attracts the eyes to the potential tumor sites. However, mucopolysaccharides can sometimes be abundant around normal adnexal structures, so the bright red color is not specific for tumor. In addition, toluidine blue is not ideal for staining squamous cell carcinomas (SCCs), which have little or no mucopolysaccharides. Another potential pitfall in staining is the introduction of a floater to the slide from a contaminant in the staining solution well. This floater would be expected at only a single locus and at a random orientation to the surgical specimen. The staining solutions should be changed frequently to minimize the risk of introducing floaters.
Mapping Tumor
The surgeon’s task of sitting at the microscope and accurately mapping tumor seen on the slides depends on the reliability of the preparation steps detailed so far. Good communication with the histotechnicians as well as daily quality assessment of at least 1 set of slides will facilitate improvement in suboptimal preparation. Specific details of orientation or problems during embedding for unusual specimens can be discussed during handoff of the slides from the histotechnician to the surgeon and may be important and/or time saving during examination of the slides. The surgeon must verify that the slides are matched with the appropriate map and that the pieces are accurately labeled and appropriately represented on the map. Generally, the Mohs surgeon scans the slide first to make sure that the epidermis, dermis, and subcutaneous fat are fully represented; the color of the staining is interpretable; and the ink is visible. Nicks are located on the section, and the location is confirmed on the map. Magnification with a ×2 objective allows the surgeon to easily scan an entire section in 1 power field. Once the tumor has been identified and confirmed with a higher-power lens, the surgeon may then review its location using a ×2 lens to facilitate accurate mapping.
Diagnostic pitfalls
A critical component of Mohs technique is the surgeon’s skill in interpreting histologic specimens ( Table 2 ). Fellowship-trained Mohs surgeons spend much of their time at the microscope acquiring dermatopathology expertise, which improves steadily in relation to the number of cases. Murphy and colleagues showed that more than 1300 Mohs surgery cases and more than 6 months of fellowship training were required before reducing errors to a minimum acceptable level of less than 1 critical error per 100 cases read. Frozen section slides may be more difficult to interpret than formalin-fixed permanent sections, and most dermatologists and pathologists have no experience in examining horizontally cut sections. The Mohs surgeon must follow a systematic, comprehensive, and reproducible system for evaluation of the frozen section slides, correlating the findings observed with the 3-dimensional specimen represented by sequential cuts. There are many challenging situations in which Mohs surgeons must be able to decide whether what they see is a malignant process or a benign structure such as an adnexal structure. Inflammatory cells can both be mistaken for a malignant process or obscure malignant cells.
| Potential Pitfall | Recommendation | |
|---|---|---|
| Floater | Floater may be introduced during curettage, making nicks, cutting, and staining | Irrigate with Saline after excision, keep the blades clean, change staining solution frequently |
| Inflammation vs Tumor | Inflammation can obscure or resemble the tumor | Examine another section from deeper in the block. Immunohistochemistry may be helpful |
| BCC vs Benign Conditions | Tangentially sectioned hair follicles can be mistaken for BCC | Examine relevant location in multiple sections |
| BCC vs Other Neoplasms | Trichoepithelioma, spiradenoma, cylindroma, MAC, and metastatic breast cancer may resemble BCC | Examine multiple sections, thaw the block and send for permanent sections. Immunohistochemistry may be helpful |
| AK vs SCC In Situ vs SCC | Misreading AK for SCC, vice versa, missing SCC clumps in the dermis | Define AK and SCC in situ and make consistent diagnosis. Evaluate the dermis carefully for small clumps of SCC cells. Immunohistochemistry may be helpful |
| SCC vs Benign Conditions | Healing wound and biopsy sites may be mistaken for SCC. Tangential sectioning of epidermis may resemble SCC | Identify biopsy site grossly and microscopically. Examine multiple sections for lumina, fragments of hair and papillae |
| SCC vs Other Neoplasms | Inflamed seborrheic keratoses and wart can be mistaken for SCC; adnexal tumors may resemble SCC | Examine multiple sections, thaw the block and send for permanent sections. Immunohistochemistry may be helpful |
| Perineural Invasion | Missing perineural invasion; Confusing with peritumoral fibrosis, re-excision perineural invasion, reparative perineural proliferation, and epithelial sheath neuroma | Have high index of suspicion in invasive SCC; Examine multiple sections; May need final full margin taken and send for permanent sections and special stains |
| Melanoma | Hard to recognize melanocytes in frozen section specimen; Inferior quality of frozen section regarding cellular detail | MART-1 staining may be helpful; good communication and close working relationship with dermatopathologist is optimal |
| Other Tumors | Skip areas in Merkel cell carcinoma, Paget disease, and sebaceous carcinoma; scar may be mistaken for DFSP; normal pilar apparatus may resemble leiomyosarcoma | Be aware of the potential false negative clear margin in multifocal tumors; consider an additional excision of margins for processing as formalin-fixed sections |
Related posts:
 Mohs Micrographic Surgery Technique
Mohs Micrographic Surgery Technique
 Mohs Surgery for Squamous Cell Carcinoma
Mohs Surgery for Squamous Cell Carcinoma
 Flaps and Grafts Reconstruction
Flaps and Grafts Reconstruction
 Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
 Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


