CHAPTER 23 Highly Cohesive Textured Form Stable Gel Implants
Principles and Technique
Summary/Key Points
Indications
The indications for primary breast augmentation that have been adopted by the authors include:
Patient Selection
During the consultation, it is imperative to evaluate several factors related to the patient’s body characteristics and her state of mind. Central to the process of selecting patients for any type of aesthetic surgical procedure is the well-being and safety of the patient. Wrongly scheduling a patient for surgery will be detrimental to the patient, the surgeon and the surgical practice. At times, the ‘best’ surgery is the one never performed.1
Medical history
In the authors’ practice, the patient’s physical health is carefully evaluated by the surgeon in charge and the anesthesiologists. Surgery can be scheduled if the medical risk of the procedure, including anesthetic, is expected to be negligible. Furthermore, if the patient has an ongoing psychiatric condition she should have documentation from her treating doctor stating that she is suitable for surgery and that the procedure will not worsen her condition.1
Patient expectations and requests
It is always the surgeon’s responsibility to inform the patient of the end result, regarding what shape is achievable, given her specific body characteristics. Involving a patient in the implant selection process without risking long-term adverse consequences requires a delicate balance. At times, patients present unrealistic expectations that make them unsuitable for surgery. An example is the very thin patient with ptotic breasts in need of a submuscular breast augmentation, but who refuses a necessary mastopexy. Another example is the patient wanting too large implants that might look disproportionate and, more importantly, exert excessive pressure on the tissue. The surgeon, together with the patient, should choose implants based on the patient’s chest wall and existing breast tissue, using different kinds of shaped implants to create the desired shape of breast. It is therefore necessary to have a thorough, ongoing discussion between surgeon and patient. The patient should be denied surgery if she requests unreasonably large implants compared with what the surgeon believes would be sound in the long term.6,7
Body dysmorphic disorder
As when dealing with any cosmetic surgical procedure, it is important to exclude patients suffering from body dysmorphic disorder, as surgery only reinforces the condition. During the consultation, it often becomes evident if a patient is suffering from body dysmorphic disorder, but at times, a few screening questions are required. If the patient has a history of bulimia or anorexia, she should have been declared healthy at least six months prior to the consultation.2,3
Patient information and education
Each patient should be made as knowledgeable as possible through extensive preoperative information. The information may, for example, be delivered through an informative web-site, verbally and in written form. If the patient is well informed prior to the consultation, the discussion between the surgeon and the patient becomes more meaningful and the patient can participate fully in the choice of implants. It is imperative that the patient understands that additional surgery might be required at some point in the future. The patient should also be aware of the risk of capsular contracture and its consequences.8
Body characteristics and implant range
In recent decades, the range of implants on the market has increased steadily. Several implant systems from different manufacturers are now available with anatomical, teardrop-shaped implants varying in height, width and projection, as well as round implants varying in diameter and projection. The sheer number of available implants and shapes might at first seem daunting, but as the chest wall shape and breast size among women in a uniform population usually do not vary greatly, a relatively small number of implants is required to solve most cases. In the authors’ experience, a majority of breast augmentations can be performed using fewer than 10 different available implants. However, given the great implant diversity, it is possible to find and fit an implant for virtually every patient’s features and desires. This allows the surgeon who is striving for perfection to challenge and solve both minor and more difficult cases involving breast and chest wall asymmetries in a way never possible before.4,5
Implant Selection
Most frequently used are the anatomical, teardrop-shaped implants.
In general, anatomical implants have their advantage in cases where a certain shape is more important than just added volume for thin patients, and for correction of breast asymmetries. The authors prefer textured implants with highly cohesive silicone gel, as these provide excellent control over the aesthetic result both in the short and long term. Furthermore, the risk of implant rupture, rippling9, bottoming out and visibility is low over time.
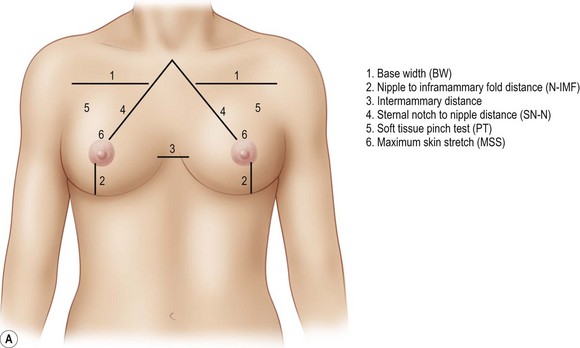
The surgeon then moves on to measuring the patient’s chest wall and breasts. The measurements should include the base width (BW), the nipple to inframammary fold (N-IMF) distance measured under maximum stretch, the intermammary distance, sternal notch to nipple distance (SN-N), a pinch test of the tissue in the breasts’ upper pole and a skin stretch test (Fig. 23.1AB).

Preoperative Planning and Marking
Positioning of IMF Incision
The senior author Dr. Randquist has developed an easy and understandable system when calculating the positioning of the implant and IMF incision by controlled lowering of the inframammary fold as illustrated in Figure 23.2






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


