Therapy for HAE is dependent on three considerations: Patients with HAE should all wear a MedicAlert disk stating the diagnosis and emergency treatment. Treatment of hereditary angioedema with a vapor-heated C1 inhibitor concentrate. Waytes AT, Rosen FS, Frank MM. N Engl J Med 1996; 334: 1630–4.
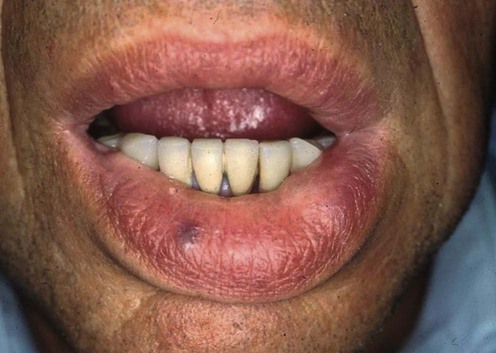
Hereditary angioedema
Management strategy
 Relief of acute angioedema, especially preservation of the airway
Relief of acute angioedema, especially preservation of the airway
 Prevention of relapse due to dental and surgical interventions
Prevention of relapse due to dental and surgical interventions
Prevention of relapse due to dental and surgical interventions
Acute Angioedema
First-line therapies
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree






 C1-INH concentrate
C1-INH concentrate