17
Hand Vascular Injuries and Digit Amputations
Vascular injuries of the hand and digit amputation can result in complete loss of function of the hand. These injuries require immediate attention by a specialist to ensure optimum functional results for the patient.
 Vascular System of the Hand
Vascular System of the Hand
Vascular competency defines the hand’s capacity to counter the stress placed on hand tissue. If a given stress outstrips the ability of the vasculature to compensate for the hand’s cellular metabolic needs, vascular insufficiency results.
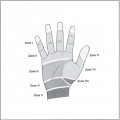
The hand is supplied with blood by the ulnar artery and the radial artery. New studies have demonstrated that the radial artery is dominant 57% of the time, whereas the ulnar artery is dominant 21.5% of the time (the two arteries are codominant the remaining 21.5% of the time [this topic is still controversial]). The radial artery divides into a small superficial palmar artery and large dorsal radial branch. The ulnar artery divides into superficial and deep branches. Next, the dorsal radial branch gives off the princeps pollicis and radial digital index branch and then anastomoses to the deep branch of the ulnar artery to form the deep palmar arch. The superficial branch of the radial artery anastomoses to the superficial ulnar artery to make the superficial palmar arch. The common digital arteries arise from the superficial arch. The digital branches arise from the common digital arteries. The vascular supply is regulated by metabolic demands, sympathetic tone, hormonal factors, and environmental factors.
Physical Examination
Basic tenets of the vascular examination of the hand include testing each digit for capillary refill, sensation, edema, color, gangrene, and petechiae. To test the proximal blood supply, take the blood pressure in both arms for a difference comparison. Next, perform an Allen’s test (see Chapter 12). If you cannot feel a pulse, then check the wrist for radial and ulnar Doppler ultrasound signals and use Doppler ultrasonography to perform an Allen’s test. Test the integrity of the palmar arches. If you are having difficulty performing a capillary refill test on the digits due to ecchymosis or avulsion of skin, you may use Doppler ultrasonography to determine the integrity of the digital vessels. For continuous monitoring of the perfusion to a finger, a pulse oximeter may be used on the involved finger.
If you are unable to perform the above exam or if the zone of injury to the vessels is in question, then an angiogram may be helpful. Finally, make sure to palpate the compartments of the forearm/hand as well as measure the compartment pressures with a Stryker needle or arterial line to rule out compartment syndrome and the need for a fasciotomy (see Chapter 19, Fig. 19–2,19–3).
Arterial Injuries
Presentation Pallor, lack of capillary refill or pulse distally, pulsatile bleeding. Intimal damage may present with late thrombosis.
Mechanism Crush, stab, or avulsion injuries
The indications for repair of radial/ulnar artery injuries are
• Absolute indication: Hand or digital ischemia
• Relative indication: Improved cold intolerance, provide better circulation for wound healing
• Digital vessel repair: Digit ischemia
Treatment
Forearm and Hand Injuries
In cases of sharp injuries to the artery, direct repair can be performed. When there has been a crush injury to the artery or an avulsion, resection of the injured portion and the use of vein grafts for reconstruction is required. Signs of vessel damage include telescoping of the vessels, petechial hemorrhages on the vessel wall, vessel thrombosis, cobwebs in the vessels, or poor flow from proximal end of the injury. In these cases, reversed vein grafts can be used. The dorsal hand veins can serve as a good donor site. If the patient requires extensive forearm fracture reduction prior to repair of the artery, Silastic (Dow Corning, Midland, MI and Barry, UK) shunts can be used as a temporary way to reperfuse the hand until the fracture is stabile. Then arterial reconstruction is performed at that setting. A forearm fasciotomy should be performed if the patient has compartment syndrome or compartment syndrome is anticipated.
Digital Arteries
It is important to note that only one digital artery is required for adequate blood flow. In fact, digital revascularization is 90% successful. However, providing a venous outflow is critical.
Cannulation Injuries
A vessel injury can often occur from cannulation of the radial artery with an arterial line or arterial blood gas sampling. This can result in pseudoaneurysm formation, thrombosis, or arteriovenous fistula formation. The rate of thrombosis in the vessel is directly correlated to the duration of cannulation. If the patient has a loss of radial pulse, but does not have any digital ischemia, surgery is not needed. The treatment of these injuries entails surgical exploration and thrombectomy with direct arterial repair. Significant vessel gaps are repaired via reversed vein grafts harvested from the cephalic or saphenous veins. An arteriogram may be beneficial preoperatively or intraoperatively to identify the level and character of occlusion.
Hypothenar Hammer Syndrome

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


