The advances in hair transplantation, particularly the advent of follicular unit transplantation, have greatly elevated the outcome of this procedure. Various modifications to the basic technique as well as innovations focused on the different aspects of the hair transplantation procedure have further enhanced this type of hair restoration surgery. In addition, there is ongoing expansion of the indications and applications of this procedure beyond the usual male pattern hair loss.
Key Points
- •
Follicular unit transplantation yields the most natural looking results and is considered as the current gold standard in hair transplantation.
- •
Basic steps in hair transplantation consist of donor area harvesting, graft dissection and storage, recipient slit creation and placement of grafts.
- •
Aside from strip harvesting, follicular unit extraction (FUE) is another newer technique in donor harvesting. Variations in the FUE technique include the use of manual, motorized and automated punches and the utilization of robotic technology.
- •
Indications for hair transplantation has gone beyond male and female pattern hair loss of the scalp to include transplanting hair over non scalp areas with hair loss such as the eyebrows, eyelashes, moustache, beard and pubic area.
- •
Scarring alopecias due to secondary causes such as burns, surgery and trauma are mostly amenable to hair transplantation however the utilization of this procedure for primary cicatricial alopecias remains controversial.
Introduction
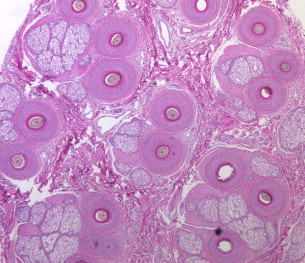
Hair transplantation has evolved throughout the years from the larger punch grafts to the smaller mini grafts and finally to the more refined follicular unit graft transplantation performed by most hair restoration surgeons today. This advancement in hair transplantation has its basis in the identification of the follicular unit as the naturally occurring structure of hair follicles on the human scalp. This histologic structure was first described by Headington as a circumscribed unit containing 1 to 4 hair follicles along with its associated sebaceous glands and arrector pili muscle insertion ( Fig. 1 ). Because follicular unit transplantation follows the aforementioned natural pattern of hair follicles on the human scalp, the procedure yields the most natural-looking results and is considered the current gold standard in hair transplantation. There are unifying concepts and general steps that characterize this type of surgery; however, there are likewise a lot of variations and innovations in the techniques and applications of this procedure.
Introduction
Hair transplantation has evolved throughout the years from the larger punch grafts to the smaller mini grafts and finally to the more refined follicular unit graft transplantation performed by most hair restoration surgeons today. This advancement in hair transplantation has its basis in the identification of the follicular unit as the naturally occurring structure of hair follicles on the human scalp. This histologic structure was first described by Headington as a circumscribed unit containing 1 to 4 hair follicles along with its associated sebaceous glands and arrector pili muscle insertion ( Fig. 1 ). Because follicular unit transplantation follows the aforementioned natural pattern of hair follicles on the human scalp, the procedure yields the most natural-looking results and is considered the current gold standard in hair transplantation. There are unifying concepts and general steps that characterize this type of surgery; however, there are likewise a lot of variations and innovations in the techniques and applications of this procedure.
Procedural techniques
The basic steps in hair transplantation, including follicular unit transplantation, consist of donor-area harvesting, graft dissection and storage, recipient slit creation, and placement of grafts. The technique of follicular unit grafting was originated by Limmer and further detailed by Bernstein and Rassman in the early 1990s. Since then, the basic procedure remains the same with some variations, modifications, and added applications.
Donor harvesting
Strip Method
Currently, the most common approach in harvesting the donor area is by surgical excision of a strip from the occipital and parietal areas of the scalp, using a single blade or a double-bladed scalpel ( Fig. 2 ). To minimize follicular transection, the blade must be held parallel to the angle and the direction of the hair shafts and excision must be made up to the subcutaneous level where the hair bulbs are located. For better visualization of the donor area, some surgeons use magnification devices, such as a loop with 1.5 to 4.0× lens magnification. The ideal donor strip should be taken from the safest and most permanent part of the donor scalp, which is, in most cases, located in between the superior and inferior border of the donor hairs.
To further decrease follicular transection, some surgeons have made some modifications to the basic technique. The Haber spreader is a device with a set of jaws with 4 sharp staggered prongs. The goal is to harvest the strip by separating the skin along the natural tissue dissection plane. A superficial scoring incision is first made to delineate the strip edges, then the instrument is inserted into the incision, and finally the handles are pressed together to separate the wound edges. Although this device may be helpful in some patients, there a certain cases when it may be difficult to separate the skin tissue with the spreader, thus, the surgeon may have to use a scalpel blade to excise the area.
Another modification to the strip harvesting method is through strip excision with the aid of skin hooks. The skin is superficially scored with a scalpel blade and then skin hooks are inserted just below the rim of the wound edges. Once inserted, the skin hooks are then lifted and pulled in opposite directions to allow direct visualization of the follicular units. A scalpel is then used to gently excise the strip without transecting the follicles.
The general guideline for obtaining donor strips that result in very thin linear scars is to obtain strips that are long and narrow. For instance, for regular hair transplantation sessions (1500–2500 grafts), the width may range from 1.0 to 1.5 cm, whereas the length would vary greatly from 20 to 30 cm depending on the patient’s follicular unit density and the total graft requirement. Another factor that influences the width size of the strip is the laxity of the donor area. The more lax the skin, the wider the strip that can be excised while still being able to close the donor wound with minimal tension.
For patients who may need more than one hair transplantation session, subsequent procedures may lead to multiple linear scars if the strips are obtained from donor areas separate from the previous scar. To avoid this from occurring, the technique is to incorporate the old scar with the current strip, thus, resulting in a single scar even after multiple surgeries. In general, the subsequent strip has to be narrower than the prior surgeries for lesser tension when closing the wound. In addition, other techniques, such as scalp massage to improve laxity and double-layer closure for wider scars, may help improve the outcome.
Closure Techniques
To close the donor wound, commonly used closure materials include nylon, polypropylene, Vicryl or monocryl sutures, or staples. Techniques include continuous single-layer closure, combined continuous and retention sutures, or the application of staples. Closure with staples may take less time to accomplish; however, patients may complain of more discomfort during the postoperative period. Here at the University of British Columbia (UBC) hair transplant center, for first-session surgeries, a continuous single-layer closure with 3-0 nylon or prolene sutures is typically performed. These nonabsorbable sutures are then removed after 1 week. For subsequent surgeries, when the donor area has less scalp laxity, a double-layer closure with absorbable monocryl or Vicryl may be used.
Trichophytic Closure
The main concern with strip harvesting is the appearance of the resultant donor scar. In most cases when the surgeon has excised a long, thin strip with narrow width (eg, <1 cm) and closure was done without tension, the donor scar would usually be very minimal. However, there are cases when wider strips may have to be excised for larger graft requirements. In addition, for most patients and surgeons, improvement of even a minimal scar has some benefit. Toward this end, Marzola, Rose, and Frechet introduced the application of the trichophytic closure in hair transplantation at about the same time period. This technique is performed after the excision of the donor strip and involves the de-epithelialization or removal of the epidermis of either the superior or inferior wound edge ( Fig. 3 A). The two sides would then be approximated together with the de-epithelialized edge underneath the other donor rim. The purpose of removing the epidermis at the wound edge is for the hair follicles, which were superficially cut, to grow within the resultant scar, thus, minimizing the appearance of the scar.
The general guideline is to perform a very superficial excision just below the epidermis not exceeding 1 mm to avoid damaging the permanent portion of the hair follicles at the area of the bulge. This coincides with the results of a study whereby morphometric analysis of the hair follicle and measurement of the depth of the bulge area was done. The mean follicular length was approximately 4.16 mm, whereas that of the bulge area was from 1.0 to 1.8 mm. The depth of the bulge area was determined through immunoreactivity of CK15, a bulge stem cell marker. Thus, to avoid damaging the bulge portion, the trichophytic cut should be less than 1 mm from the surface of the skin.
The instruments used to remove the edge varies, with some surgeons advocating the use of a scalpel to make a right-angle edge, whereas others use scissors. Observed effects of the trichophytic closure revealed that there can be problems with resultant hair angles, more so with superior edge de-epithelialization, thus, inferior edge removal is preferred. For surgeons using the trichophytic closure technique, improvement in the appearance of the resultant donor scars is observed in many patients (see Fig. 3 B).
Follicular Unit Extraction
With the natural looking results of follicular unit transplantation over the recipient area, more attention is being given to improving the scars at the donor area. Although properly done donor strip excision commonly results in minimal linear scars, some surgeons and patients prefer less visible, nonlinear scars. Thus, another technique in donor harvesting, known as follicular unit extraction (FUE), was introduced. The basic procedure involves identifying a follicular unit at the donor area and extracting the individual follicular unit via a punch devise. Variations in the FUE technique are discussed later. Although a linear scar is not produced, this procedure still results in scars that usually appear as dotted hypopigmented macules over the donor area. The proponents of this procedure have put forth other advantages, such as less postoperative pain over the donor area and the ability to obtain grafts from patients with very tight donor skin caused by multiple surgeries. Critiques of this procedure include potentially high transection rates that may occur with the blind extraction of individual grafts and much longer completion times. And because this procedure is operator driven, a successful outcome would largely depend on the skill of the surgeon.
Manual Punches
The FUE procedure basically uses punches that range from 0.8 to 1.5 mm in diameter. Punches may also have sharp or dull tips, with the choice of tip dependent on the technique preferred by a particular surgeon. One of the main techniques described by Rassman and colleagues is the FOX procedure, which uses a sharp 1-mm punch to make a superficial incision up to level of the mid-dermis followed by the extraction of the individual follicular unit with a forceps. Not all patients are good candidates for this procedure; thus, the proponents of this technique have proposed the FOX test, which is a test session to determine transection rates and, hence, identify which patients would yield positive results.
Another modification of the FUE technique is the Surgically Advanced Follicular Extraction system described by Harris. In this procedure, first a sharp punch creates a superficial scoring incision, which is then followed by a blunt dissecting punch to separate the follicular unit from the surrounding tissue. A variation is the use of a serrated dull tip. A study on patients with male pattern hair loss showed transection rates of 6.14%, with a range of 1.7% to 15.0%. A potential side effect of this procedure is the possible occurrence of buried grafts with the use of dull tips.
Motorized and Automated Punches
Punch devices used for FUE now include motorized and automated punches, such as the automated FUE and implantation system NeoGraft (Medicamat, Malakoff, France). This machine uses pneumatic pressure and automated control to extract individual follicular units. The physician controls the harvesting hand piece, which has a rotating and cutting canula for excision of grafts. After extraction, the grafts are suctioned into a canister. Trimming of the grafts are not necessary. Multiple punch diameter sizes with a depth limiter are provided. Another feature of this machine is the implantation handpiece. A combination of pneumatic pressure automatically loads the graft into the implantation canula then implants on the recipient site as directed by the physician. The surgeon still has to manually create the recipient slits using regular methods, after which the handpiece can then be used to insert the grafts. A study of 40 FUE cases comparing manual and powered FUE punches showed that the mean harvesting time of the latter group was faster at approximately 100 grafts per 8.9 ± 1.3 minutes. The transection rate reported was 5.5%.
Robotics
Trying to address the disadvantages of FUE, such as long procedural times and high transection rates, a company has come up with a robotic machine (ARTAS System, Restoration Robotics, Mountain View, California) to extract grafts. This machine has recently obtained approval by the Food and Drug Administration. This FUE system has an image-guided set of cameras and computer programming to improve accuracy in extracting follicular units. Physicians control the settings of the machine. The multiple cameras first capture images of the scalp, and then the computer’s software analyzes the data through complex algorithms and computations. Through the aforementioned process, the system maps out and monitors the follicular unit location and patient motion. The computer-guided robotic arm with a 1-mm needle and blunt punch then harvests at random based on the follicular unit spacing set by the physician. Their reported transection rate is less than 10% and the extraction rate is 500 to 600 grafts per hour. The surgeon and/or nurses then implant the grafts manually after the recipient slit creation using hypodermic needles or miniblades.
Lin X and colleagues reported another hair-harvesting robot with an end-effector arm. This machine has a digital microscope that first localizes and determines follicular units and then guides the punch with a motorized shifting mechanism and rotary guidance design to harvest grafts. The reported end-effector bias and precision was 0.014 mm.
Nonscalp Donor Area
There are patients who are not considered good candidates for hair transplantation because of a poor scalp donor area. Some may have depleted donor supplies from previous hair transplantation procedures. For this subset of patients, there is a need for additional sources of donor supply. Alternative sources from other hair-bearing areas of the body may provide an expanded pool in a select group of hirsute individuals. FUE of nonscalp hairs has been performed by some surgeons with moderately good outcomes. In a case report, this procedure was done because of the extensive scalp scarring with limited donor area. Chest hairs served as donor grafts for the recipient scalp. After more than 1 year, there was acceptable transplanted hair growth. Another observation was the change in length of the chest hairs from 4 cm to and 15 cm (4 times) at about 1.5 years after the hair transplantation.
In another case series whereby some patients had severely depleted donor areas caused by previous surgeries, grafts were sourced from chest, abdomen, beard, arm, and leg areas. There was a reported 80% to 85% survival of the transplanted grafts. In this study, procedural details included the shaving of the donor areas 1 week before surgery to ensure extraction of anagen hairs and the use of hypodermic needles customized at the tip and mounted on a rotary tool as the punch device. The cases had, on average, around 1500 to 1800 grafts per session, with several 2 to 3 consecutive daily sessions done to achieve the total graft requirements. The aforementioned patients were very hirsute individuals, thus, allowing for the extraction of a large number of grafts.
The success of this type of procedure depends heavily on the skill of the surgeon. Other disadvantages include hairs of lesser quality when compared with scalp hairs (eg, caliber and length differences). Although there are some reports of an increase in the length of the transplanted hairs, other surgeons were not able to observe this finding. In certain patients, the body hair supply may be insufficient. In terms of the best source of nonscalp hair, the beard area would most likely yield grafts with the potential to grow longer than the hairs from the other areas of the body.
Hair Regeneration from Bisected Follicles
To further expand the donor supply, various studies have looked into the growth potential of bisected or partial follicular units. A study by Toscani and colleagues bisected hair follicles horizontally resulting in upper and lower portions. The upper part was cut just below the insertion of the arrector pili muscle and was approximately one-third of the length from the dermal papilla. The donor hair follicles were then implanted on the recipient area of a patient with male pattern hair loss. Both the upper and lower portions were stained for epithelial stem cell markers. The hair regrowth evaluation done after 1 year revealed the presence of epithelial markers CD200, beta 1 integrin, and p63 detected over both portions, signifying the possibility of a reservoir of progenitor stem cells capable of regenerating an entire hair follicle. Hair regrowth was 72 ± 0.4% of the transplanted upper portions and 69.2 ± 1.1% of the lower portions. The hairs from the bisected follicles had slightly finer caliber hairs compared with intact hairs.
Another study extracted partial longitudinal follicular units. The vertically divided hair follicles (100 and 150 grafts) extracted from the occipital areas of 5 patients were transplanted into their respective recipient areas. After 1 year, there was a mean growth of 95.9% of the partial follicular units transplanted on the recipient area, with the growing hairs possessing the same characteristics as the donor hair.
Graft dissection and handling
After the hair-bearing strip is harvested from the donor area, it is cut into slivers of 1 to 2 rows of follicular units ( Fig. 4 ). These slivers are then further dissected into follicular unit grafts with 1, 2, 3, or 4 hairs, depending on the observed natural grouping of the follicular units on a patient’s scalp ( Fig. 5 ). Proper dissection into follicular unit grafts involve carefully trimming the tissue surrounding the follicular units, thus, ending up with a pear-shaped graft that is wider at the base where the bulbs of the follicles typically splay and narrower at the top where the hairs converge as they exit the skin. Instruments used for the slivering and dissecting of follicular unit grafts commonly include the number 15 or 10 scalpel blades or double-edged razor blades depending on the training and preference of the surgical assistants.




