Superior hair restoration requires the application of universal principles along with variations that apply to specific ethnic populations. This article serves as a primer on basic tenets of hair restoration, with additional attention given to the uniqueness and differences in technique and design that are warranted for a wide range of races and ethnicities. This article also gives prospective surgeons an insight on how to undertake further study and shore up their deficiencies so as to refine knowledge gaps and ensure patient safety and excellent surgical outcomes.
Superior hair restoration requires the application of universal principles along with variations that apply to specific ethnic populations. This article serves as a primer on basic tenets of hair restoration, with additional attention given to the uniqueness and differences in technique and design that are warranted for a wide range of races and ethnicities. Because hair restoration is a complex subject that mandates sophisticated understanding pertaining to the process of hair loss and how to restore lost hair, this article is not intended to provide a broadly encompassing knowledge to enable full engagement in a safe, clinical practice dedicated to hair transplant surgery. However, this article gives prospective surgeons an insight on how to undertake further study and shore up their deficiencies so as to refine knowledge gaps and ensure patient safety and excellent surgical outcomes.
Although this article is geared toward surgeons, like with any surgery, one must first understand when not to operate before one can claim the right to operate on an individual. In short, this brief introduction rapidly outlines cogent limitations that any surgeon must appreciate and understand before starting a practice in hair restoration surgery.
First, hair loss is a progressive disease that involves an expanding region of baldness with dwindling usable hair to transplant into this bald region. (The principle of modern hair restoration is predicated on Norman Orentreich’s seminal work in the 1950s that showed that hair grafts transplanted from a region genetically programmed not to be lost, that is, the back and sides of the head, will not be lost even when transplanted into a region that is genetically programmed for hair loss.) One of the greatest fears for transplant surgeons is that they will run out of usable hair to complete the process of hair restoration. This is particularly pertinent in the case of a younger patient with rapidly progressive hair loss, mainly a male patient in his 20s who reveals a pattern that is most likely to become an advanced Norwood class VI or VII. It is the ethical responsibility of every surgeon to understand that hair transplantation in a young male patient is fraught with risks that should be emphasized to the patient, for example, the depletion of donor hair, leaving the surgery unfinished or unnatural results, need for multiple sessions during the patient’s lifetime, and the inability to completely shave the head because the donor scar will be revealed. Considering the complexity of the requirements for safe hair restoration in a young patient, the authors advise that the novice surgeon primarily considers medical management as a treatment of choice for young patients.
Medical management of hair loss
With pitfalls in mind, one must understand the indication for medical treatment for any male patient who is suffering from hair loss. Because hair loss is a progressive disease, medical treatment is required even for the individual who is contemplating hair restoration surgery; it consists of Food and Drug Administration–approved medications, such as minoxidil (Rogaine) and finasteride (Propecia). These medications slow the progression of hair loss. Their major limitation, other than ongoing cost, is that once they are stopped, the patient’s hair loss will revert to the starting pattern, that is, everything he gained during the period he was on the medications is lost.
Although the authors have no options currently besides surgery to restore hair, the results obtained from the use of medications are still significant. Further, medical treatment is most effective in the younger patient with early signs of miniaturization (to be discussed), less effective in patients with more advanced settings of hair loss, and almost completely ineffective in patients who demonstrate “slick baldness” (ie, not even a wispy hair remains). However, medical management offers the ability to restore miniaturized (or vellus) hairs back into thicker, terminal hairs and to slow down the progression of hair loss. Accordingly, even in patients who are contemplating hair restoration, medical management can serve as a potent adjunct to limit further loss and thereby maintain the transplant result to maximal effect, that is, add to the transplanted hairs by maintaining the surrounding original hair.
The nature of male pattern baldness has been discussed in this section. Most men do not advance from thick, terminal hairs to complete baldness. Instead, thick, terminal hairs are slowly converted over time to wispy, vellus hairs (baby hairs) that in turn are shed and lost. Medical management works to reconvert a portion of this type of hair back toward thicker, terminal hairs. Once the hairs are completely gone, they do not grow back. That is why early implementation of medical management is important for anyone who is beginning to lose hair.
Finasteride is an inhibitor of dihydrotestosterone (DHT), which locally causes follicles to miniaturize and shed. Finasteride is an oral medication taken at a dosage of 1 mg/d to retard further hair loss. It is processed through the liver and reduces one’s prostate specific antigen by roughly 50%; anyone taking finasteride should alert his or her primary care physician to this fact. It has a very low incidence of sexual side effects, which are reversible on cessation. Finasteride is contraindicated in premenopausal women for risk of birth defects in the male fetus; a woman of childbearing age should not ingest it or handle any crushed pills. Finasteride has shown equivocal benefit in postmenopausal women. It generally takes about 6 to 12 months to start seeing appreciable changes after the start of finasteride.
Minoxidil is a topical medication to be applied to the scalp (not hair) twice a day. Its mechanism of action is unclear, but it is known to convert hairs from the telogen phase into active anagen phase. Accordingly, at times, some hair shedding occurs early in the first few weeks after starting the application as hairs move from telogen to anagen, which should be explained to the patient. Results can be seen earlier in the first few months after the start of minoxidil than with finasteride. The major limitation of minoxidil is contact dermatitis, which can be virtually eliminated in patients who use the brand named Rogaine Foam, which removes the propylene glycol irritant.
Female hair loss considerations
More than 30% of women older than 30 years also lose hair even before the onset of menopause. Women can lose hair in a male pattern, diffusely across the hair or in a Christmas tree pattern in which the apex of the “tree” falls along the vertex and the base along the frontal hairline, as described by Olsen. The major problem with hair restoration in women is the need to first understand the underlying process that could account for the hair loss, because although hair loss is predominantly genetic in men, it is not so for women. Besides a small number of females in whom hair loss is genetic, the other reasons for hair loss are usually divided into 2 types: dermatologic and hormonal. Dermatologic evaluation by a dermatologist would be indicated in a woman who exhibits any unusual skin disease that could account for the problem at hand. Basic hormonal workup is indicated in almost every woman to rule out treatable, reversible hormonal diseases, such as hypothyroidism, iron deficiency anemia, autoimmune disorders, and other hormonal imbalances. If no other underlying process is causing hair loss, the first choice of treatment for female hair restoration is 2% minoxidil. The application is topical, the indication is twice a day, and the patient should be alerted to possible initial hair shedding. If the patient is considering hair transplantation, it is highly suggested that she use minoxidil for at least 4 to 6 months before undergoing surgery.
Female hair loss considerations
More than 30% of women older than 30 years also lose hair even before the onset of menopause. Women can lose hair in a male pattern, diffusely across the hair or in a Christmas tree pattern in which the apex of the “tree” falls along the vertex and the base along the frontal hairline, as described by Olsen. The major problem with hair restoration in women is the need to first understand the underlying process that could account for the hair loss, because although hair loss is predominantly genetic in men, it is not so for women. Besides a small number of females in whom hair loss is genetic, the other reasons for hair loss are usually divided into 2 types: dermatologic and hormonal. Dermatologic evaluation by a dermatologist would be indicated in a woman who exhibits any unusual skin disease that could account for the problem at hand. Basic hormonal workup is indicated in almost every woman to rule out treatable, reversible hormonal diseases, such as hypothyroidism, iron deficiency anemia, autoimmune disorders, and other hormonal imbalances. If no other underlying process is causing hair loss, the first choice of treatment for female hair restoration is 2% minoxidil. The application is topical, the indication is twice a day, and the patient should be alerted to possible initial hair shedding. If the patient is considering hair transplantation, it is highly suggested that she use minoxidil for at least 4 to 6 months before undergoing surgery.
Dermatologic contraindications to surgery for hair loss
This section discusses the broad classification of hair loss diseases that are contraindications for surgery, such as scarring alopecias (eg, discoid lupus, central centrifugal alopecia, traction alopecia), nonscarring alopecias (alopecia areata), and psychological conditions (eg, trichotillomania), and how to recognize these conditions. The surgeon who wants to enter the field of hair restoration surgery and who does not have an in-depth dermatologic background must undergo careful study of these diseases so as to avoid surgery in those patients who are not safe candidates. In addition, surgeons can use their dermatologic colleague and internist more effectively when they encounter a situation that would suggest a contraindication to surgery.
Techniques in hair transplant surgery
After understanding the medical side of hair loss, the surgeon should now exercise artistic and technically precise hair restoration techniques. Unlike other types of esthetic surgeries, excellent hair restoration is completely dependent on an excellent surgical team. Likened to building a car, the entire team is important for the success of the outcome. The surgeon’s role typically involves deciding on the proper surgical candidate, preparing the donor area for harvesting, designing the hairline, harvesting and closing the donor area, and creating the recipient sites for the eventual hair grafts. The surgical team must perform excellent hair-graft dissection and hair-graft placement. Without these 2 very important components, the hair transplant result can look unnatural or show poor growth. This short section principally focuses on the surgeon’s role during hair restoration and briefly touches on the technique of graft dissection and placement. In addition, a focus on the differences in technique as directed toward ethnic populations would be an important consideration, given the emphasis of this presentation.
Hairline Design
The hairline height and shape exhibits the surgeon’s artistry and technical knowledge of hair restoration at its zenith. Hairline design is also one of the most important differentiators among various ethnicities, which will be explored in depth after a basic understanding of good hairline design that is more universal in scope is outlined.
The hairline resides at the junction between the horizontal and the vertical plane of the scalp, more specifically at the 45° intersection between these 2 planes. This intersection is the lowest acceptable starting point (central point) for any hairline (but can be scaled upward based on age and degree of existing or projected hair loss) because any hair transplanted below this point corresponds with forehead scalp, which should remain bare. The lateral extent of the anterior hairline falls along an imaginary line drawn through the lateral canthus (lateral points). Hair that resides lateral to this point signifies temporal hair, which also finishes the facial frame and can be as important as the anterior, horizontal hairline in establishing a youthful and balanced result. Once the central point and the 2 lateral points have been fashioned, the points are joined by creating a suppressed saucer-shape design where the central region extending from the central point to the midpupil is flat, from the midpupil toward the lateral canthus is forward convex in design, and the lateral extent beyond lateral canthus point slightly concave to meet the temporal hairline. The degree of suppression and the roundness of the design are based on multiple factors. The younger patient who does not have significant hair loss may tolerate a slightly less-suppressed frontotemporal recession, whereas an individual with more advanced loss would benefit from a more recessed frontotemporal design.
The hairline variations described here pertain to the male hairline; as mentioned earlier, female hair restoration has authentic characteristics and thus lies beyond the scope of this discussion.
Caucasian males tend to exhibit frontotemporal recession. Even in younger patients, the shape of hairline should have some degree of frontotemporal recession designed to accommodate further aging and associated hair loss so that the hair design remains natural over time. It is recommended to design a conservatively high midpoint and receded frontotemporal angles to ensure adequate supply of donor hair needed to cover the increasing demand versus supply ratio occurring in further hair loss progression. With that in mind, the conservatively positioned hairline can be safely lowered in subsequent procedures, but it is very difficult to raise it after establishing a lowered, surgically created one. The reverse temptation is also true for many starting surgeons, that is, to start a hairline so far back that there is no beneficial frame to the face, and thereby the esthetic contribution of hair to the face is lost. Therefore, designing a hairline that is not too high or not too low is a work of art and requires good esthetic judgment.
At the opposite extreme of the hairline for the Caucasian male, an African male exhibits a hairline that is almost straight or straight across forehead with no visible frontotemporal recession (ie, almost a right angle at the frontotemporal junction). A greater degree of recession at this angle is indicated in the advanced balding African male who has limited donor hair but not as limited as his Caucasian counterpart. Because a pronounced frontotemporal recession does not look natural and because shaved hairstyles offer a socially acceptable alternative for the African male (and for other races also), surgical hair restoration may not be a suitable option for a young patient with rapid hair loss. Donor-strip harvesting that creates a visible scar in the closely cropped head must be discussed in advance with a prospective patient, especially with one who may have limited donor hair, ongoing hair loss, and the need to replace an ever-widening field of alopecia, because the strip harvesting may prevent the option of a shaved hairstyle.
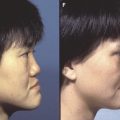
Asians tend to have rounder and wider heads, and their hairlines similarly should match this design with a wider arcing central convexity and less-pronounced frontotemporal recessions (with the judgment based on the degree of hair loss and head shape) ( Fig. 1 ). The shape of Asian hairline is “flat-convex” in comparison with the Caucasian “round-convex” hairline.