Introduction
The groin flap, nourished by the superficial circumflex iliac artery (SCIA), is historically important because it was the first successful free flap. With its concealed donor site, this flap was especially popular in children and young women. However, it is less commonly used nowadays due to the anatomic variations in the course and size of the pedicle vessels that make flap elevation difficult. With the recent development of perforator flaps, the major pedicle vessels of musculocutaneous and fasciocutaneous flaps could be left in place at the donor site and the flap could be harvested based on branches of these vessels only, thus minimizing donor site morbidity while preserving reliable blood supply with the flap. Additionally, musculocutaneous flaps could be replaced with cutaneous perforator flaps of the same skin territory, by dissecting the perforator vessels away from the muscle fibers that they traverse, and allowing for preservation of maximal function at the donor site. Similarly, fascia could be left in place at the donor site where it would have been included with the flap in standard fasciocutaneous flaps.
All these modifications are performed today, without a significant decrease in the skin territory size and blood supply included with the flap. This concept of perforator flaps has been applied to the development of the superficial circumflex iliac artery perforator (SCIP, skip) flap, which is based on a perforator with a small segment of the superficial circumflex iliac vessel. This chapter covers both the traditional groin flap and the SCIP flap and discusses modifications of both these flaps.
Flap Anatomy
Arterial Supply of the Flap (see Figs 43.1 and 43.2 and Fig 11.3 , Fig 11.6 , Fig 11.8 , Fig 11.9 , Fig 11.10 )
The region of the groin and the surrounding areas (lower abdomen and upper thigh) are supplied by the superficial circumflex iliac artery (SCIA), the superficial inferior epigastric artery (SIEA), the deep circumflex iliac artery (DCIA), and the lateral circumflex femoral artery (LCFA). The SIEA supplies the lower abdominal area, the DCIA supplies the superior lateral area of the anterior superior iliac spine (ASIS), and the LCFA supplies the anterolateral thigh region. The SCIA is present in 98% of cases and is usually at least 1 mm in diameter. In some cases, if the SCIA is small and the SIEA is large, the SIEA can be used to supply the same region. The SCIA is the main supply to the region and, unless it is absent or too small, it is the vessel of choice for harvesting the region of the groin.
Dominant:
superficial circumflex iliac artery (SCIA)
Length: 2 cm (range 1.5–3 cm)
Diameter: 1.5 mm (range 0.8–2 mm)
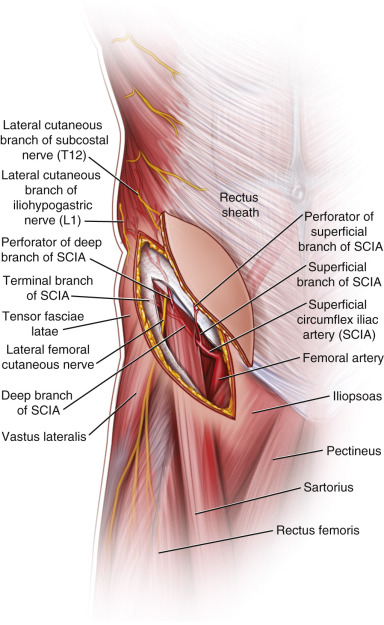
The SCIA takes off from the anterolateral aspect of the superficial femoral artery approximately 3 cm below the inguinal ligament and runs laterally approximately two fingerbreadths below and parallel to the inguinal ligament. It originates from a common trunk with the SIEA (one-third of cases). It gives off a superficial branch that is located proximally over the deep fascia of the sartorius muscle and distally in the fatty tissue. It gives off a few perforators (0.3–0.5 mm caliber) at the middle portion of the anteromedial groin region.
The deep branch of the SCIA system runs in a superolateral direction beneath the deep fascia of the sartorius muscle through the inguinal ligament. After penetrating the deep fascia at the lateral border of the sartorius muscle, the deep branch enters the suprafascial layer to give off several perforators (0.5–0.8 mm caliber) in the anterolateral portion of the groin region.
When a superficial branch is long and large, the deep branch is usually short and small. Sometimes, in cases in which the superficial branch is absent, only the long and large deep branch can be detected. The distal terminals of the superficial and deep branch sometimes connect to the perforators from the deep circumflex iliac system, deep inferior epigastric system, and the lateral circumflex femoral system.
Venous Drainage of the Flap (see Fig. 43.2 and Fig 11.6 , Fig 11.8 )
The region of the groin is drained by two main systems: superficial and deep. The superficial circumflex iliac vein (SCIV) and the superficial inferior epigastric vein (SIEV) constitute the superficial system, and the venae comitantes of the different arteries constitute the deep system. The SCIV and SIEV are usually located superficial to Scarpa’s fascia. In many cases, these two veins join to form one large vein (2.5 mm diameter) that can be used for anastomosis. Additional veins in the regions are perforating veins of concomitant veins of the DCIA, and perforating veins of the transverse branch of the LCFA system.
Primary:
superficial circumflex iliac vein
Length: 3 cm (range 2–4 cm)
Diameter: 1.8 mm (range 1.5–2 mm)
Secondary:
concomitant vein of the SCIA system
Length: 2.5 cm (range 2–3 cm)
Diameter: 1 mm (range 0.5–1.5 mm)
These veins are significantly smaller than the superficial system. They can be anastomosed directly to a recipient vein or they can be connected to the superficial system if the venous system does not seem to drain the flap adequately. Usually one concomitant vein is present, and sometimes there are two. Veins from the surrounding systems can be used as secondary drainage of the flap as long as the flap encompasses these veins.
Flap Innervation ( Figs 43.1 and 11.10 )
Sensory:
The region of the groin is supplied by T12 and L1 segmentally. Although not commonly performed, using the lateral cutaneous branch of T12 allows a sensate flap to be harvested.
Motor:
The flap cannot include any motor potentials; however, if the sartorius muscle flap is included, the motor nerve to the muscle can be included with the flap (this is rarely performed).
Flap Components
The fascia lata or fascia of the abdominal wall, adipose tissue, iliac bone, or lateral femoral cutaneous nerve can be included in this flap. The sartorius muscle may be included based on perforators of the SCIA that supply the upper portion of the muscle. In cases with penetration of the SCIA through the sartorius muscle, flap elevation is easier if part of the sartorius muscle is included.
Advantages
Groin Flap and SCIP Flap
- •
Minimal donor site morbidity
- •
Donor site is easy to conceal
- •
A large cutaneous vein is available as a venous drainage system
- •
Reliable blood supply
- •
Lateral portion of the flap can be thin
SCIP Flap
- •
Deeper and longer dissection of the SCIA system to the femoral artery, as in the groin flap, is unnecessary
- •
Only the dominant perforator and a short length of the superficial or deep branch is required to nourish the flap
- •
Flap elevation time is short
- •
Thinning of the flap may be done with primary defatting
- •
Thinning to create a customized adiposal flap with volume reduction may be done in one stage
Disadvantages
Groin Flap and SCIP Flap
- •
Bulky, particularly in the medial aspect of the flap
- •
Short pedicle and small vessels
- •
Significant anatomic variation of the vessels
- •
Presence of pubic hair, particularly in the medial aspect of the flap
SCIP Flap
- •
Supermicrosurgery is necessary to dissect and to anastomose the smaller and short pedicle vessels
- •
There is an anatomic variation of the SCIA system: when the pedicle perforators of the free SCIP flap are hypoplastic or smaller (<1.0 mm), smaller recipient vessels are necessary for anastomosis.
Preoperative Preparation
Designing and marking the course of perforators are essential components of a successful perforator flap transfer. The high degree of anatomic variation within the SCIA system is widely known, and contributes to the perception that SCIP flap surgery is particularly difficult. The SCIA system is sometimes hypoplastic or missing, requiring the reconstructive strategy to be altered during surgery, so it is important to know preoperatively which artery is dominant in this region. Prior knowledge of any hypoplasia or hyperplasia in the SCIA, SIEA, and DCIA systems within a groin region promotes the ease and safety of SCIP flap surgery.
Preoperative color Doppler ultrasound (US) evaluation is very useful for planning the SCIP flap. CT angiograms are not suitable for delineating the course of the superficial and deep branches of SCIA system, owing to the short perforator length of the major vessels in this lesion. The handheld Doppler system is similarly inferior to color Doppler US in preoperative identification of SCIP flap perforators because it cannot provide precise information on the subcutaneous tissue layer.
Male patients need hair trimming around the groin region. There is no age limitation but the flap is best suited for young females and children.
Flap Design ( Fig. 43.3 )
Anatomic Landmarks
The pubic tubercle, anterosuperior iliac spine, inguinal ligament, and femoral artery are marked. Color Doppler US examination confirms the course of the SCIA, which runs parallel to and 2–3 cm below the inguinal ligament. If a SCIP flap is to be harvested, the dominant perforator of the superficial and deep branches of the SCIA system is usually located at the cross-point 3 cm medial to the anterior superior iliac spine along the course of the SCIA.
General Thoughts About Flap Design
Wide flaps should be avoided in patients with thick adipose tissue, as donor site problems may occur.
In designing a SCIP flap, the point of the ASIS should be included in the design of the flap. The flap can be extended beyond the ASIS toward the back in a superolateral direction.
If a very large flap is to be harvested, it is beneficial to include the SIEA system. Other dominant arterial systems such as the DCIA or deep inferior epigastric artery (DIEA) can carry the groin region in cases in which the SCIA system is hypoplastic.
After locating the vessels supplying the flap, the skin paddle size and design should be adjusted based on the location and size of the vessels. This applies more to the SCIP flap in which the perforator is preferably centered within the flap markings. Larger flaps can be harvested if the artery is large, dominant, and pulsatile.
A different version of the flap, the lateral islanded groin flap, is harvested from the more lateral aspect of the groin. The purpose is to extend the pedicle length and to harvest a thinner flap. The medial marking of the flap begins lateral to the femoral triangle and extends laterally. A T-shaped incision is made with the T lying on its side.
The osteocutaneous groin flap based on the SCIA is designed as described for the standard groin flap; however, a segment of iliac bone is included in the design. The ASIS is preferable left at the donor site to minimize contour deformities.
Special Considerations
In defects of the extremities with small recipient vessels, the SCIP flap or the groin flap can both provide vessels with a suitable match in size.
The surgeon can plan the design and axis of the flap to allow for inclusion of the SIEA in case the SCIA cannot be found or is too small.
Differences in Design, if Any, When Performing the Flap as Pedicled or Free
Dissection of the pedicled flap does not require visualization of the pedicle or extensive dissection of the pedicle, as long as the arc of rotation is adequate. In order to increase the arc of rotation, pedicle dissection can be performed.
Flap Dimensions
Skin Island Dimensions
Length: 15 cm (range 10–20 cm)
Width: 10 cm (range 5–15 cm), maximum to close primarily: 10 cm
Maximal dimension: posterior margin, 10 cm lateral to anterior superior iliac supine.
Superior border: umbilical level.
Inferior border: 10 cm below the inguinal ligament
Muscle Dimensions
A small segment of sartorius muscle proximally can be harvested with this flap if necessary.
Bone Dimensions
Length: 4 cm (range 3–8 cm)
Width: 2 cm (range 1–3 cm)
The iliac bone can be harvested based on the SCIA; however, it is better harvested based on the deep circumflex iliac vessels.
Flap Markings ( Fig. 43.3 )
Groin and SCIP Flap
The ASIS and pubic tubercle are marked and a line is drawn connecting the two landmarks. A line is drawn two fingerbreadths (approx. 3 cm) below and parallel to the inguinal ligament. This is the line of the vascular pedicle. The superficial femoral artery is palpated in the femoral triangle.
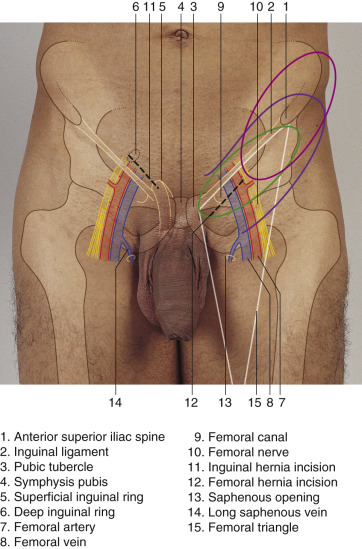
The flap is centered over this line and can be extended 5–10 cm lateral to the ASIS. The width can be up to 10 cm, with primary closure being possible.
SCIP Flap
The SCIA perforator exits around the medial aspect of the anterior superior iliac spine. The flap is marked lateral and medial to the perforator with more of the extension laterally.
Patient Positioning
The preferred position is supine. There is no need to place a bump below the hip as the anatomy may become distorted and the pedicle may be under tension during harvest.
Flap elevation is difficult but feasible in the lateral decubitus position.
Anesthetic Considerations
If necessary, a small flap can be elevated under local anesthesia. Epidural or lumbar anesthesia is sufficient for flap elevation.
Technique of Flap Harvest
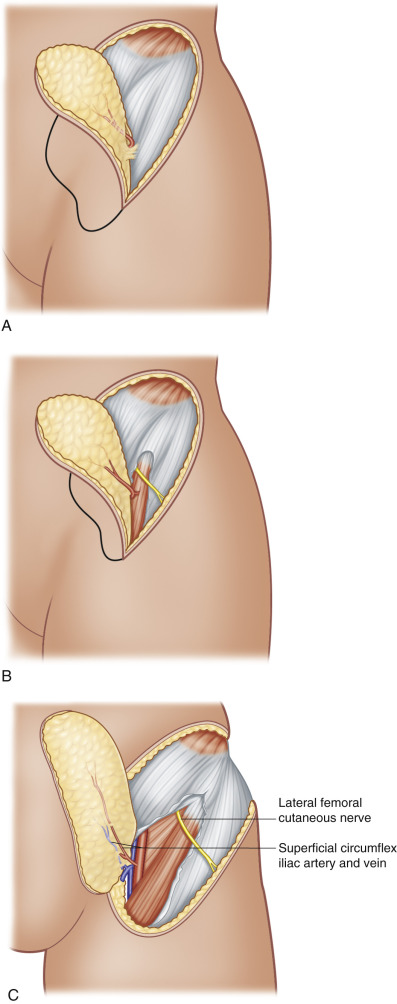
Groin Flap ( Fig. 43.4 )
Pedicled Groin Flap
The dissection is begun on the lateral aspect and continued medially. On the lateral aspect of the flap, the incisions are made down to the fascia lata, the inguinal ligament, and the external oblique, and the dissection is carried medially superficial to these fascial structures. As the dissection proceeds medially, the sartorius muscle becomes visible under the fascia. Care is taken to visualize the pedicle as the dissection approaches the lateral border of the sartorius muscle. The flap is dissected deep to the fascia of the sartorius muscle in order to avoid injury to the deep branch of the SCIA. Once the medial aspect of the muscle is encountered, flap dissection is stopped. Only if necessary, the flap is dissected medially beyond the medial aspect of the fascia of the sartorius muscle. If this is necessary, the flap is harvested as if it were a free flap (see below).