Chapter 52 Table 52.1 Gracilis muscle/musculocutaneous flap, innervated flap
Gracilis Muscle/Musculocutaneous Flap, Innervated Flap
Flap |
|
Tissue | Muscle or muscle with skin paddle |
Course of the vessels | Underneath the muscle distally after entering the muscle laterally |
Dimensions | 4–6 × 20–25 cm (muscle); 6–8 × 10–12 cm (skin island) |
Extensions and combinations | — |
Anatomy |
|
Neurovascular pedicle | — |
Artery | Terminal branch of the medial femoral circumflex artery |
Veins | Concomitant veins of the medial femoral circumflex artery |
Length and arc of rotation | 6–7 cm |
Diameter | Artery, 1.2–1.8 mm; vein, 1.5–2.5 mm |
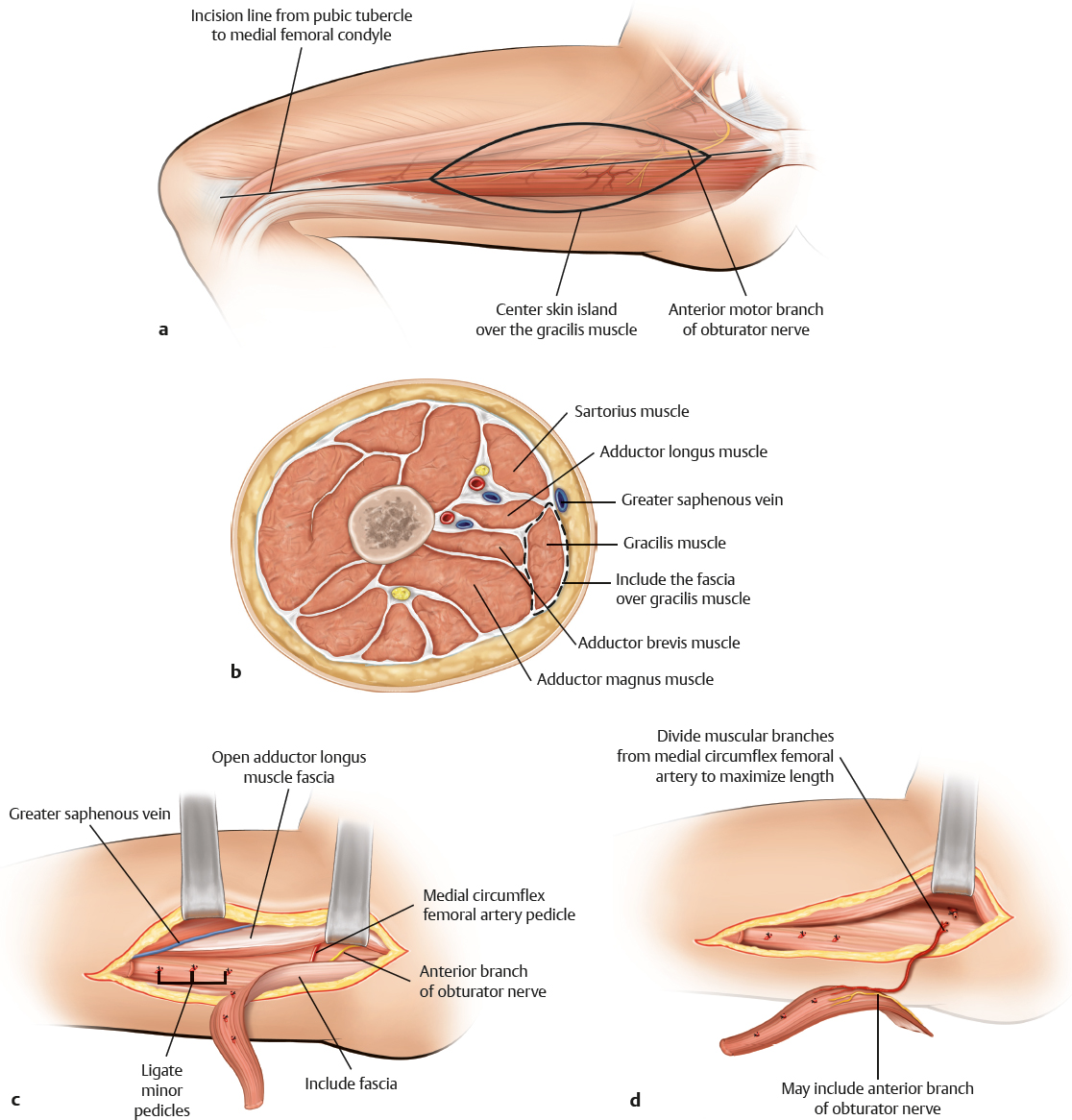
Nerve | Anterior motor branch from the obturator nerve |
Surgical technique |
|
Preoperative examination and markings | Draw a line from the pubic tubercle to the medial condyle; the prominence of the adductor magnus marks the superior border of the gracilis |
Patient position | Supine, with the hip and knee flexed and the leg abducted |
Dissection | Incise 2 cm inferior and parallel to the line drawn preoperatively; do not violate the greater saphenous vein (anterior to the incision); incise the fascia; identify the gracilis muscle; divide the muscle distally; ligate the minor pedicle; proceed with the dissection cephalad; retract the adductor longus by moving proximally; expose the pedicle 6–12 cm distal to the pubic tubercle; protect the medial cutaneous nerve on the surface of the adductor magnus; clip or ligate small branches; divide the muscle superiorly; check for perfusion and then transfer the flap. NOTE: Center the skin island over the middle of the proximal portion; incise down to the fascia; include the fascia lata in the dissection; identify the muscle and proceed as above |
Advantages |
|
Vascular pedicle | Short but reliable; vessel size is sufficient if the pedicle is dissected to maximal length |
Flap size and shape | Long flat muscle with suitable cross-section area to serve as functional muscle transplant |
Combinations | Skin island |
Donor site | Minimal donor site morbidity with acceptable scar |
Disadvantages |
|
Flap | Distal skin island is not reliable |
Pearls and pitfalls |
|
Dissection | Do not confuse the gracilis and sartorius muscles; do not dissect the skin island too anteriorly; the gracilis is always more dorsal than projected; perform good muscle excursion for functional replacement |
Extensions and combinations | — |
Contouring and correction | Rarely required; sometimes needed with bulky skin islands |
Clinical applications | Long narrow defects for coverage alone; functional muscle transfer for loss of muscle groups |