Gluteal Flaps for Sacral Pressure Injuries
Terri A. Zomerlei
Jeffrey E. Janis
DEFINITION
Sacral pressure injuries are common in chronically supine patients.
Patient populations most at risk include those in acute care settings, nursing home patients, and paraplegic populations.
In addition to unrelieved pressure, the causes are multifactorial and may include incontinence/moisture, friction/shear force, and altered sensory perception.
Characteristically, the appearance of the overlying skin represents only a small portion of the affected tissue (“the tip of the iceberg”).
ANATOMY
The sacrum is a large concave triangular bone at the base of the spine that is the fusion of sacral vertebrae S1-S5.
A pressure injury develops as a result of unrelieved pressure between the sacral bone and the sitting or lying surface.
The gluteus maximus muscle is a broad, thick, quadrangular muscle that forms the prominence of the buttocks.
The gluteus maximus originates along the posterior gluteal line of the ilium and the lateral aspect of the sacrum, coccyx, and sacral ligaments.
The superior portion of the muscle inserts along the iliotibial tract of the fascia lata, and the inferior portion of the muscle inserts into the greater trochanter of the femur.
It is a type III muscle with two dominant blood supplies, the superior and inferior gluteal arteries.
The vessels arise separately from the internal iliac artery.
The arteries exit the pelvis with their respective venae comitantes and the superior and inferior gluteal nerves.
The anatomic landmarks for locating the neurovascular pedicles are the piriformis muscle, the posterior iliac spine, the greater trochanter, and the ischial tuberosity.
The superior gluteal artery exits above the piriformis one-third the distance from the posterior iliac spine along a tangent from the posterior iliac spine to the greater trochanter.
The inferior gluteal artery exits below the piriformis just lateral to a point half the distance between the posterior iliac spine and the ischial tuberosity (FIG 1).
PATHOGENESIS
Primary mechanism of pressure injury is cellular ischemia.
Tissue pressure greater than the pressure of the microcirculation (32 mm Hg) causes ischemia.
If the ischemic period is long enough and repeated frequently, the eventual outcome is tissue necrosis.
Pressure injuries (decubitus ulcers) almost invariably occur in the tissue over bony prominences in persons not able to change body position frequently.
Pressure injuries overlying the sacrum are common in chronically supine patients.
In acutely ill patients, third-space fluid may mechanically compromise the microvasculature.
Etiologic considerations can be divided in extrinsic and intrinsic factors.
Extrinsic factors: Primarily mechanical forces on the soft tissues
Friction: Resistance that a surface encounters when moving over another; most often occurs with patient transfers
Moisture: Incontinence can lead to skin breakdown.
Pressure: Mechanical force that is applied perpendicular to a plane (ie, between a bony prominence and a chair or bed)
Shear: Mechanical stress parallel to the plane results in stretching and compression of the blood supply to the muscles and skin.
Intrinsic factors: Patient factors that affect the soft tissues
Altered level of consciousness: Results in lack of voluntary movements and protective reflexes that off-load pressure
Anemia: Can contribute to fatigue and weakness which can perpetuate immobility.
Autonomic control: Decreased levels result in spasms, perspiration with increased skin moisture, blood vessel
engorgement with resulting tissue edema, and problems with bowel and bladder control.
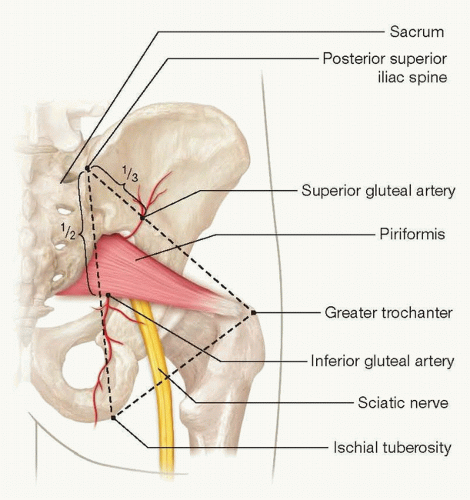
FIG 1 • Sacral anatomy.
Age: Increasing age is associated with increased skin friability and decreased tensile strength.
Diabetes: Poorly controlled blood glucose levels are associated with early recurrence of pressure injuries.
Infection: Profoundly impairs wound healing abilities.
Inflammation: Creates a hostile local milieu resulting in impaired healing, especially in the setting of chronic wounds.
Malnutrition: Results in wasting and decreased muscle bulk and impairs wound healing abilities
Sepsis: Can result in decreased tissue perfusion and ischemia
Sensory loss: Patient is unable to experience the discomfort associated with prolonged pressure over prominences.
NATURAL HISTORY
Pressure injuries are categorized according to the National Pressure Ulcer Advisory Panel Stages.
Pressure injuries can progress through the following stages if extrinsic and intrinsic insults are not remedied (FIG 2).
Stage I: Intact skin with nonblanching erythema
Stage II: Partial thickness skin loss with exposed dermis
Presents as a blister, abrasion, or shallow open ulcer
Stage III: Full-thickness skin loss
Subcutaneous fat may be exposed.
Tunneling and undermining may be present.
Stage IV: Full-thickness skin and tissue loss
Unstageable: Full-thickness skin or soft tissue loss but depth is unknown usually due to the presence of an overlying eschar
Suspected deep tissue injury: Blood-filled blister or deep purple discoloration of intact skin may indicate deep tissue injury that needs to evolve prior to staging.
HISTORY AND PHYSICAL FINDINGS
The preoperative evaluation of patients with any type of pressure injury includes a detailed assessment of the patient’s medical history, social situation, and baseline health status and a comprehensive wound evaluation.1
Patient history
How long has the pressure injury been present? Acute wounds may respond to conservative treatment, whereas chronic wounds tend to be more recalcitrant.
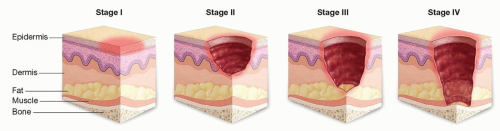
FIG 2 • Pressure injury staging.
What is the current wound care treatment? Changing local wound care regimens may help with improving the wound.
What surgical options have been tried in the past? Obtain any and all operative reports as previous surgeries may limit surgical options.
Is the patient ambulatory, or wheelchair or bed bound? Some flap procedures are not appropriate for ambulatory patients.
What type of mattress and turning regimen is currently being used? Airflow mattresses offer the best protection, whereas normal mattresses offer little defense against pressure.
Is fecal contamination a problem? A dressing or a temporary diverting ostomy may be prudent.
Are there problems with urinary incontinence? A urinary diversion procedure (ie, suprapubic tube) or indwelling Foley catheter may be indicated.
Does the patient have spasms? Optimize medications to control spasms.
Does the patient have any fixed contractures?
What is the baseline nutritional status of the patient?
Social history is crucial to obtain in order to understand possible postoperative barriers to care and to thwart recurrence.
What is the social support/caregiver situation?
Do they have resources for obtaining durable medical equipment (low air loss bed, seat cushion if bed bound or wheelchair bound)?
Is there smoking or substance abuse history?
Active or prior nicotine use increases risk of poor wound healing.
A urine toxicology screen or urine cotinine test may be useful.
Is there a history of psychiatric illness?
Does the patient follow a specific diet (cardiac, diabetic)?
What is their daily protein intake?
What is the patient’s compliance history?
Laboratory studies
Complete blood count to assess for anemia or active infection
Albumin, prealbumin, and total protein to assess protein stores
Coagulation panel to assess for coagulopathies
Cultures that should be obtained with tissue or bone biopsies as wound swabs have little value due to chronic colonization. Cultures should be sent for quantitative analysis, and if the organism count is greater than 105, consideration should be given to systemic antibiotics and/or staged debridement and reconstruction.
Urinalysis
Physical exam
All wounds must be examined manually.
Visual wound assessment alone is not sufficient to obtain necessary information about a wound.
Manually assess the size and depth of the wound, bony prominences, bursa, proximity to the rectum, and presence of tunneling (may need to use long cotton tip applicator to assess tunneling).
If an eschar is present, the wound cannot be accurately staged.
A limited bedside debridement may be useful, if the patient can tolerate this, so that the wound can be staged and to facilitate local wound care preoperatively.
From visual inspection, take note of any previous surgical scars as previous surgeries may preclude the use of a flap secondary to compromised vascular supply.
Muscle tone and bulk are assessed taking note of any spasticity or contraction of the extremities.
Assess the patient’s sensation in the area of the wound.
IMAGING
MRI is recommended for all stage IV pressure injuries to evaluate for osteomyelitis.
T2 hypersensitivity and low-intensity T1 is sensitive and specific for osteomyelitis (97% and 89%, respectively).
If MRI is not available or the patient has conditions precluding its use, plain films and CT scan may be used. This imaging can be confirmatory for osteomyelitis but has low specificity.2
DIFFERENTIAL DIAGNOSIS
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


