Introduction
The word glabrous is defined as “smooth, having a surface without hairs or projections.” Anatomically, glabrous skin is present on the palms of the hands and volar fingers, as well as the plantar surface of the feet and toes. Replacing glabrous skin on the hand and fingers is best accomplished by microneurovascular transplantation of similar skin from the foot, most often from the great toe. A “pseudo-glabrous” surface can be created with transplantation of muscle and split-thickness skin graft (STSG) for coverage of large palmar defects. This pseudo-glabrous surface is relatively insensate but feels smooth and has the septal qualities of glabrous skin.
For palmar defects, we prefer muscle and STSG to fasciocutaneous flaps. Non-glabrous skin flaps, fasciocutaneous flaps, or venous flow-through flaps give excellent cover but do not have the unique septal support of finger and thumb tips. Certainly, replacing “like with like” is the first choice in reconstructing a surgical wound, but glabrous donor tissue is limited and is reserved for smaller defects. For instance, an entire palm cannot be resurfaced with a glabrous donor site because of the lack of availability. An exception would be an unusual case of “spare parts” surgery, where donor amputated tissue is present that cannot be replanted. Non-glabrous tissues have drawbacks: these flaps do not have the density of nerve fibers, and therefore less chance for fingertip quality reinnervation; they may be hair-bearing; and their color match may be inconsistent.
This chapter focuses on the great toe and second toe pulp neurovascular island flaps and medial plantar instep neurovascular island flaps, which all provide glabrous skin on a consistent vascular pedicle. The toe pulp flap can be used to resurface distal digital pulp wounds, while the instep flap can provide a larger area of tissue approaching the size of an entire volar finger or a comparable-sized palmar defect.
Regional Anatomy (see Fig 13.7 , Fig 13.8 , Fig 13.11 , Fig 13.15 , Fig 13.16 , Fig 13.17 , Fig 13.19 )
Arterial Anatomy of the Region (see Figs 13.15 and 13.17 )
Arterial blood supply to the foot and toes comes from either the posterior tibial or anterior tibial system. The anterior tibial artery becomes the dorsalis pedis artery over the dorsum of the foot under the extensor retinaculum. At the level of the proximal first metatarsal interosseous space, the dorsalis pedis bifurcates, sending the first dorsal metatarsal artery along the dorsal aspect of the interspace between the first and second metatarsal and a second communicating branch that travels deep. This branch perforates the interspace to communicate with the plantar system.
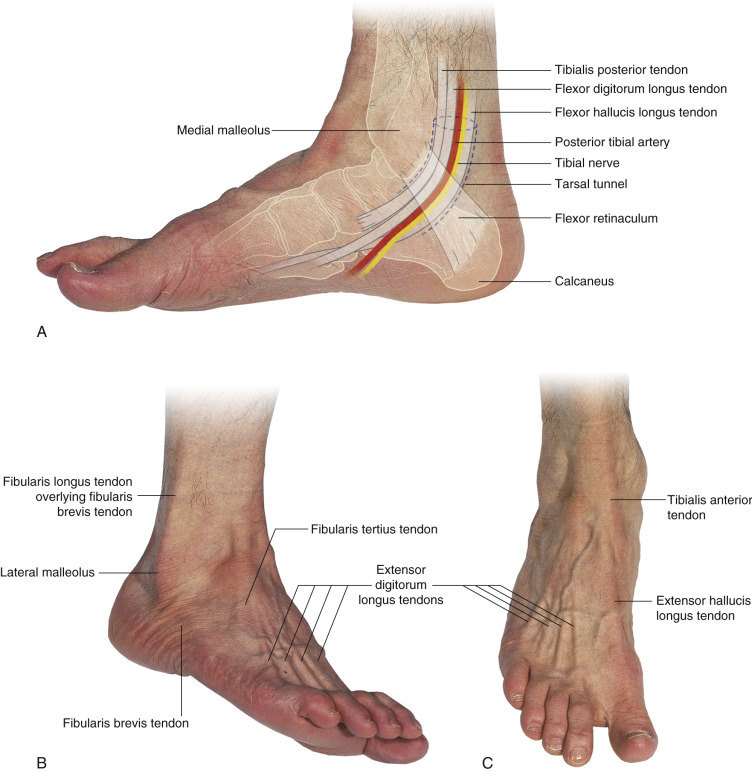
The posterior tibial arterial system enters the foot posterior to the medial malleolus of the tibia in the tarsal tunnel. This artery then bifurcates into medial and lateral plantar arteries, with the medial plantar branch further subdividing into several branches. The lateral plantar branch joins the plantar system at the level of the base of the metatarsal. Multiple common digital arteries branch at this level and travel deep to the metatarsal and eventually join the dorsal metatarsal arterial system just distal to the transverse metatarsal ligament. At this junction, the artery immediately bifurcates, sending terminal digital artery branches both medially and laterally.
At the level of the first cuneiform the medial plantar artery divides into several branches. The medial branches communicate with the dorsalis pedis, while perforators come through the intermuscular septum between the abductor hallucis and flexor digitorum brevis to supply the medial plantar perforator flap.
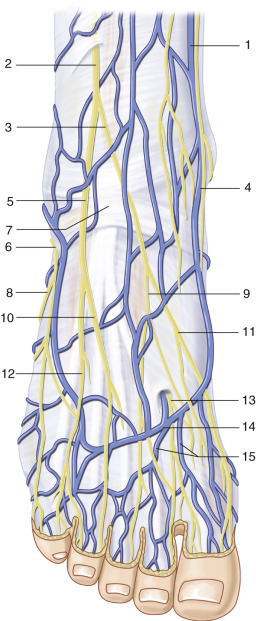
Venous Anatomy of the Region ( Figs 53.1 and 13.19 )
Small veins over the dorsum of the great and second toe coalesce into tributaries that connect to a venous arch on the dorsum of the foot, the completeness of this arch being variable. These veins run in the subcutaneous system just under the dermis and in the fatty tissue above the deep fascia of the foot, superficial to the extensor tendons. The venous arch drains into the dominant saphenous system. Long venous pedicles on any foot flap can be harvested with the saphenous system for a vein of virtually any length necessary. A second deep venous system of small venae comitantes accompanies the proper digital arteries to the toes but is generally too small for microvascular transplantation. If these veins are traced proximal to the posterior tibial artery or dorsalis pedis artery, they are larger and can sometimes be used for microvascular repair. The subcutaneous veins are, however, much larger and more amenable to microsurgical repair in most cases.
The medial plantar perforators are accompanied by venae comitantes and are able to drain the medial plantar flap. These vessels are traced back to a large branch of the medial plantar system to allow for the size necessary for microsurgical repair. Although they are comparable in diameter to the medial plantar artery, the medial plantar comitans vessels are quite thin and more difficult to handle. Another option for venous drainage is to trace a superficial vein back to the saphenous system or a large branch and use this thicker-walled system for venous drainage. Either system is adequate to decompress the arterial inflow.
Nerves in the Region (see Fig 13.7 , Fig 13.8 , Fig 13.11 , Fig 13.15 , Fig 13.16 , Fig 13.19 )
Sensory nerve supply to the plantar aspect of the foot and toes comes from the posterior tibial nerve.
The medial side of the foot is supplied by the medial plantar nerve, one of the branches of the posterior tibial nerve, the other being the lateral plantar nerve. The medial plantar nerve supplies sensation to the great toe, second, third, and medial side of the fourth toe. The plantar digital nerves lie just plantar to the digital arteries.
Branches from the medial plantar nerve or saphenous nerve may course through the medial plantar flap; whereas these nerves are inconsistent in their supply to the flap and we have not generally used them, they can potentially innervate the medial plantar flap.
Great Toe Pulp Flap and Second Toe Pulp Flap
Flap Anatomy
Arterial Supply of the Flap ( Case 1 , Fig. 53.4 , see Figs 13.15 and 13.19 )
The blood supply to the great toe pulp and second toe pulp flaps can be either dorsal or plantar dominant, depending on the patient’s anatomy. The dorsal system is dominant in 60% of cases. The dorsal system is technically simpler to dissect than the plantar system, although it can sometimes run deep between the first and second metatarsals, complicating the dissection. The plantar system is slightly more difficult to expose because it lies deeper and plantar foot exposure is more tedious with a patient in supine position.
Dominant:
first dorsal metatarsal artery or plantar metatarsal system
Length: first dorsal metatarsal 3 cm (range 3 cm to very long if traced to the anterior tibial artery); plantar metatarsal 2.5 cm (range 2–3 cm)
Diameter: first dorsal metatarsal 1 mm (range 0.5–3 mm); plantar metatarsal 1 mm (range 0.5–3 mm)
If the first dorsal metatarsal artery is traced to the anterior tibial artery, then the surgeon must be certain that the posterior tibial artery can supply circulation to the foot. This can be done with preoperative angiography or an Allen’s test of the foot.
The dorsal and plantar arterial systems join just distal to the transverse metatarsal ligament, in the first web space. At this point, small digital arteries branch laterally and medially. The branch going laterally becomes the medial digital artery of the second toe. The branch going medially at the first web space becomes the lateral digital artery of the great toe.
Minor:
first dorsal metatarsal or plantar metatarsal system
When one system is dominant, the other is considered the minor blood supply.
Venous Drainage of the Flap ( Fig. 53.1 )
Primary:
dorsal venous branches of the great saphenous vein
Length: 3 cm (range 3 cm to as long as the saphenous vein can be traced)
Diameter: 3 mm (range 3–6 mm)
Finding adequate venous drainage for the great toe or second toe neurovascular island flap can be difficult at times. Venous drainage is more prominent over the dorsum of the foot and toes.
Secondary:
venae comitantes of the first dorsal metatarsal artery and proper digital arteries
Length: 3 cm (range 3–5 cm)
Diameter: 0.5 mm (range 0.25–3 mm)
Although extremely small, these veins can be preserved and traced to superficial system branches. The superficial system in continuity with the deep venae comitantes can then be used for microsurgical repair and drainage. These veins can be used as the only drainage system if they are adequate in size for repair and have not been damaged by dissection.
Flap Innervation ( Fig. 53.1 and Fig 13.8 , Fig 13.15 , Fig 13.19 )
Sensory:
the plantar digital nerve of the great toe supplies the toe pulp. The plantar digital nerve of the second toe supplies the second toe.
The plantar nerves lie just plantar to the digital artery. The skin landmark is just plantar to the midaxial line of the toe. When dissecting in the interspace between the great and second toes, the nerve is usually first visualized and the smaller digital artery can be found slightly dorsal to the nerve.
Flap Components
The neurovascular island flap from the pulp of the great toe is a sensory cutaneous flap of glabrous skin. Other components can be added by expanding the flap to include nail, bone, etc. (see Flap modifications, below.)
Advantages
- •
Excellent choice to replace glabrous skin loss of the thumb or fingertips.
- •
If the flap is designed to be no wider than 2 cm, then the donor site can be closed primarily. The donor site may require a skin graft if the harvested flap is larger, thus prolonging patient recovery considerably.
Disadvantages
- •
Harvesting this flap can be technically demanding and inset of the flaps requires microsurgical skills.
- •
The surgeon often needs to harvest a thick flap in order to make sure that the artery is incorporated in the flap dissection. Therefore the flap can often be bulky on the thumb or finger and may require a second operation to debulk it.
Preoperative Preparation
In general, we use the ipsilateral toe as the donor toe as this lines up better when using the ulnar digital artery of the thumb as a recipient artery. If the patient has had a traumatic injury to the foot or toe, then the surgeon should consider using the contralateral toe.
A Doppler examination of the foot and toe will help demonstrate whether the toe arterial supply is plantar or dorsal dominant. We start by identifying the Doppler arterial signal of the dorsalis pedis artery and follow the signal distally. If the signal disappears at the level of the base of the metatarsal, then we can often predict that the toe arterial supply is plantar dominant. If we can hear the signal distal to the base of the metatarsal and the level of the communicating arterial branch, then there will be a usable dorsal arterial system. An arteriogram of the foot is unnecessary in most cases. We use a Doppler examination to assess the dominance of the vascular system. A good signal on either the plantar or dorsal side reassures the surgeon that a viable system will be found on dissection. Arteriography can be predictive but vasospasm in angiography of the lower extremities is often present, limiting visualization. Intra-arterial injection of a dilating agent can be useful. Magnetic resonance angiography is a newer technique, but distal vessels of small caliber can be difficult to assess. Our preference is the pencil Doppler.
Flap Design
Anatomic Landmarks ( Fig. 53.2 and Cases 53.1, 53.2 and 53.3 )
The first metatarsal artery is located between the first and second metatarsal bones.
Flap Markings and General Thoughts About Flap Design ( Figs 53.4–53.6 )
- •
The flap is designed as an oval with the long axis along the midaxial line of the lateral aspect of the great toe. If the surgeon wishes to use the second toe pulp, creating a bilobed flap, or if the second toe donor is preferable for whatever reason, marking of the oval on the medial second toe can be performed.
- •
To achieve primary closure of the donor site, the flap should not be any wider than 2 cm. If primary closure cannot be completed, a small skin graft can be used, or healing by secondary intention of the areas that have excessive tension on closure is an option.
- •
The oval is usually 3–4 cm long.
- •
The dorsal side of the oval marking should be designed to incorporate enough skin between the lateral nail margin and the incision to get good suture purchase for skin closure. Incision markings should continue proximally from the proximal margin of the oval to the web space and at that level should be extended both dorsally and in a plantar direction to identify dorsal and plantar arteries.
- •
One can base a skin flap over the medial side of the second toe based on the medial digital artery of the second toe or a larger skin flap from the lateral side of the great toe based on the medial digital artery of the great toe. The medial digital artery of the great toe is small and sometimes from a lifetime of walking can be scarred.
- •
Venous drainage of the dorsum of the foot and toe should be marked out preoperatively by having the patient hang the leg over the bed or chair in a dependent position. In this position, indelible ink should be used to mark veins, especially looking for veins draining the lateral side of the great toe.
- •
When the dorsal system is dominant, the dissection is simpler. A longer pedicle can be included with the flap, and a shorter incision is needed on the plantar surface of the foot which diminishes rehabilitation time.
Special Considerations
The oval flap can be used to reconstruct a skin/soft tissue defect in a finger. Taking the flap in combination with nail or in continuity with phalangeal bone can aid in reconstruction of complex composite defects. If a secondary soft tissue defect is present in the hand, this flap can be combined with a dorsalis pedis or even an extensor brevis flap. However, insetting and folding can be difficult and the surgeon must be wary of kinking the vascular pedicles to a chimeric flap.
Flap Dimensions
Skin Island Dimensions
Length: 3 cm (range 1–4 cm), maximum to close primarily: 4 cm
Width: 1.5 cm (range 1–2.5 cm), maximum to close primarily: 2 cm
In order to achieve primary closure, the flap width should not exceed 2 cm. Using the second toe requires that less width be harvested, because primary closure is more difficult.
Patient Positioning
The patient is positioned supine with an arm table for the injured arm and hand. A well-padded tourniquet is placed on the thigh and the upper arm.
Anesthetic Considerations
We prefer general anesthesia since we are generally working in two teams, on both the hand and the foot. A bupivacaine block is performed at the foot and toe after the flap harvest and closure for postoperative pain control. The block is performed by infiltrating adjacent to the superficial and deep peroneal branches on the dorsum, at the proximal plantar wound subcutaneously, and adjacent to the digital nerves. A block can be performed of the median and ulnar nerves at the wrist if necessary, but we are very careful not to inadvertently injure the recipient artery or vein. We have not performed this procedure under regional block.
Technique of Flap Harvest (see Cases 53.1 and 53.3 )
With the patient successfully anesthetized, if the recipient site is in the hand or contralateral foot, two operative teams work simultaneously, one team at the foot and one at the recipient site. At the hand, the operative team dissects out the recipient nerve, artery, and vein. Usually, there are abundant veins on the dorsum of the thumb and hand. The arterial blood supply usually is the ulnar digital artery; if this is not available, then the incision is extended proximally to the dorsal radial artery at the anatomic snuff box. The nerve should be the ulnar digital nerve of the thumb in reconstruction of thumb pulp. If this is not available, nerve grafts or transfer of the radial digital or distal dorsal radial nerve may be necessary.
At the foot, the second operative team makes the appropriate skin markings as described earlier. The first incision should be near the proximal end of the marked oval flap, extending proximally to find any small tributaries in the subcutaneous tissue that may drain from the flap area. In so doing, if there is inadequate venous drainage in that area, then the position of the oval may need to be altered to extend more dorsally. Once the venous tributaries are identified, then dissection can be carried out more proximally, identifying the major draining vein. The dissection can be extended proximally onto the dorsum of the foot if venous length is necessary. By this time, the surgical team at the hand should be able to determine the length of vein needed there. Once the vein has been identified, an incision continues into the web space and dissection is taken down through skin and subcutaneous tissue into the web space, identifying the lateral digital nerve to the great toe. This usually is on the plantar side of the digital artery. Once the digital nerve is identified, the artery supplying the toe will then be identified, and dissection of the artery is carried out proximally until we find communication between the dorsal and plantar systems. We also identify the medial digital artery of the second toe; eventually this branch to the second toe will be ligated and divided.
Care is taken at this juncture to identify either a plantar-dominant or a dorsal-dominant arterial system. If there is a dorsal-dominant system, then dissection is carried out proximally to whatever length is needed at the hand. As stated previously, approximately 40% of the time, we are not able to use the dorsal system, in which case we must carry out our incision more onto the plantar surface of the foot in between the first and second metatarsals, and dissect the plantar artery through this area. Dissection of the plantar digital artery can be tedious as often it will be encased in firm tissue at the level of the sesamoid over the metatarsal head. If a long arterial pedicle is needed and dissection of the plantar digital artery is difficult, we may just ligate the plantar artery and extend the arterial pedicle with a vein graft between the recipient artery and the plantar artery of the flap.
Once the plantar artery, vein, and nerve are identified and dissected proximally, the rest of the incision can be carried out, both dorsal and plantar around the previous markings. Dissection of the flap should be carried out through skin and subcutaneous tissue, identifying the major branches that go into the skin from the lateral digital artery supplying the flap. Sometimes the flap needs to be made quite thick and dissection has to be carried out all the way down to the distal phalanx of the toe. This can make for a relatively bulky flap that may be more difficult to inset. Split-thickness skin grafts are often necessary to adequately close the recipient site at the thumb and to cover the pedicle. Often, the flap does not have to be this bulky if we can identify the small perforators going into the flap from the digital artery. We can then ligate any other branches that are deep to the arterial pedicle. This part of the dissection can be very tedious and time-consuming, but is perhaps the most critical portion of the dissection.
Once the flap is elevated and isolated on the neurovascular bundle, then the tourniquet is released. The flap should become pink with arterial flow within a few minutes.
Once we are sure of adequate perfusion of the toe and we see good capillary refill and flow out of the vein, we then ligate the arterial artery, and then the vein, and then divide the digital nerve.
Special Instruments
Special instrumentation is not required for flap harvest or inset unless bone is taken to make a composite flap. The small area of bone and lack of rigidity in the toes make osteotomes difficult to use and we therefore use a micro air-oscillating saw. One must be very careful not to injure the vascular pedicle.
Flap Modifications
- •
Web space flap
- •
Toe wrap-around flap
- •
Combined lateral aspect of great toe flap and medial aspect of second toe flap
- •
Combined lateral great toe, web space, and medial second toe flap.
Donor Site Closure and Management
We close the donor site with absorbable sutures in the space between the toes since non-absorbable sutures are difficult to remove in this area. Non-absorbable sutures can be used in the plantar and dorsal foot. A dry dressing is placed and no splinting is required. The patient must be non-weight-bearing on the surgical site for 3 weeks. Special shoes can be made for bearing of the weight on the heels if the patient feels they cannot walk on their heel and avoid digital pressure.
If the donor site is closed under tension and capillary refill of the toe appears to be affected, i.e. the toe is ischemic or poorly perfused, sutures are removed until the toe becomes pink, and a skin graft is placed.
Technical Tips to Optimize Outcomes and Avoid Complications
- •
Care must be taken immediately after skin incision to find the small venous tributaries that drain the lateral or medial aspect of the great toe or second toe, respectively.
- •
We generally use papaverine liberally over the area, especially the arterial side, to reduce any segmental spasm. If spasm is not reversible by papaverine, then we look for side branches that have not been clipped or tied off. These may be a source of spasm.
- •
Care must be taken to include a vein that drains the toe pulp flap during the initial dissection of the flap.
Flap Usage
Pedicled
A neurovascular island flap from the great toe pulp is almost always used for reconstruction of lost pulp from the thumb or fingertips. We have also used this as a pedicled flap for closure of wounds over the plantar surface of the foot over the metatarsal head. The arc of rotation can reach both the first and second plantar metatarsal regions.
If considering this as a donor to a foot wound in a patient with a chronic non-healing wound, be aware that, if a local wound cannot heal, it may be that the toe will not heal either.
Free Flap
- •
Thumb pulp reconstruction: the skin, pulp, artery, vein, and nerve must be used.
- •
Finger pulp reconstruction: the skin, pulp, artery, vein, and nerve must be used.
- •
Palmar, thenar, or hypothenar defects: the nerve need not be used if no recipient area nerve is available.
We do not use this flap in the lower extremity, trunk, or head and neck region.
Typical Indications for the Use of This Flap
Toe Pulp for Volar Thumb Reconstruction
At the hand, the operative team dissects out the recipient nerve, artery, and vein. Usually, there are abundant veins on the dorsum of the thumb and hand. The arterial blood supply usually is the ulnar digital artery, but, if this is not available, then the incision is extended proximally to the dorsal radial artery at the anatomic snuff box. The nerve should be the ulnar digital nerve of the thumb in reconstruction of thumb pulp. If this is not available, nerve grafts or transfer of the radial digital or distal dorsal radial nerve may be necessary.
The flap is dissected as described and the flap is then brought to the recipient field, where it is then inset with some loose tacking stitches. The artery is then repaired either end-to-end with the digital artery or end-to-side or end-to-end with the dorsal radial artery at the anatomic snuffbox, using the operating room microscope and either 9 or 10-0 nylon.
The vein is then repaired end-to-end to a branch of the cephalic vein. The digital nerve is usually repaired after circulation has been established. The wounds are then closed relatively loosely.
We are liberal with the use of STSG, even over the pedicle. We use a venous Doppler probe on the outflow vein to determine if there is an inflow and outflow circuit established into the flap. We have seen several of these neurovascular island flaps take a few days to become fully pink. There may be some arterial venous shunting that takes place early on after the microvascular anastomosis is completed.
The donor site is closed in layers. Because of the tightness of the skin closure, the toe will actually look pale for the first day or so. If the closure is so tight that there is no flow to the toe, we suggest placing a skin graft and then, at a later date, approximately 6 months postoperatively, resecting the skin graft and trying to close the wound secondarily, if the patient wishes.
Soft tissue defects on the thumb or fingertips, where sensation is important and glabrous skin has been lost, are ideal for this type of reconstruction. We ensure that the recipient area is clean and free of debris or any sign of infection. In cases of tumor resection, reconstruction can be performed immediately, if it is certain that tumor margins will be free. If margins are pending, the hand/finger wound can be addressed and reconstructed when permanent sections have established clear margins.
Technique
Under tourniquet control, the reconstruction is begun by finding a suitable recipient artery, usually a digital artery, princeps pollicis in case of the thumb or a common digital artery. The artery should be out of the zone of injury and free from significant trauma. Flow can be checked when the tourniquet has been released. A vessel that freely squirts blood from the lumen in a pulsatile fashion is considered adequate.
The digital nerve is found, preferably outside the scar bed. It is transected and bulging fascicles are found. The digital nerve adjacent to the artery is typically used. The hand is turned over and a dorsal vein on the finger or more proximally is found outside the zone of injury. The size of the vein should be compatible with the toe vein or slightly larger.
When the donor is ready, it is brought into the field and partially inset. This allows the arterial pedicle, nerve, and vein to be aligned for repair. After repair under the microscope, the wound is closed. If closure is tight, a skin graft is used so as not to compromise arterial inflow or venous drainage.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


