Chapter 13 Genioplasty
Summary
Introduction
The chin is the lower topographic limit of the face and thus plays an important role in the perception of appropriate facial proportions.4,5 A vertically deficient or excessive chin places the lower third of the face out of balance relative to the middle and superior thirds of the face.6 Horizontal deficiency or excess diminishes facial pulchritude, most notably in profile (Figs 13.1 & 13.2). Additionally, the chin has a pivotal role as a reference in the appreciation of other facial features, most notably the nose. A large nose is often paired with a deficient chin and they have a reciprocally negative effect on the appearance of each other and on overall facial attractiveness (Fig. 13.3).7–9



Improvements in the chin can be achieved by osteotomy or by the use of implants or grafts for augmentation.10 Osseous procedures include burr reduction (ostectomy), osteotomy with caudal segment repositioning, osteotomy with grafting or osteotomy with segmental sectioning.11–15 Augmentation genioplasty can be accomplished with autologous tissue grafts such as bone or cartilage or, more commonly, with alloplastic implants.16,17 The benefits of alloplastic augmentation include a shorter and less technically demanding procedure. However, alloplastic genioplasty can pose limitations in achieving large augmentation without causing lip retraction, has a lower success rate for correction of asymmetry and offers very limited potential to change the vertical dimension of the chin.18
Anatomy
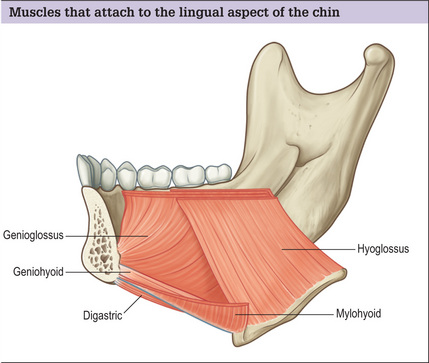
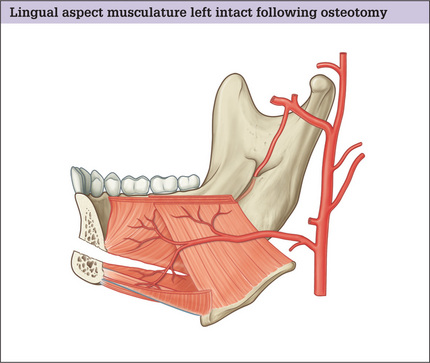
From external to internal, the layers of the chin include skin, subcutaneous fat, muscles, periosteum and bone. The depressor angularis, depressor labi inferioris and mentalis attach to the anterior plane of the chin. The geniohyoid, genioglossus, mylohyoid and anterior belly of the digastric attach to the lingual aspect. Following elevation of the anterior periosteum and horizontal osteotomy, the blood supply of the caudal chin segment is maintained via terminal lingual artery periosteal perforating branches that travel through the musculature attached to the lingual side (Figs 13.4 & 13.5).
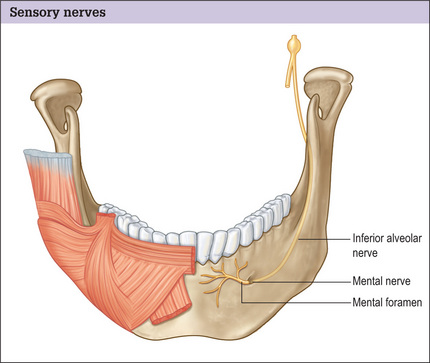
The mental nerve supplies sensation to the anterior mandibular gingiva, mucosa and lower lip. It is a continuation of the inferior alveolar nerve and exits the mandible via the mental foramen. The mental foramen is located in the vertical plane between the first and second mandibular premolars. In the terminal portion of its course, as it travels posterior to anterior, the nerve ascends to the foramen (Fig. 13.6). This upward trajectory must be understood when planning the location and angle of a horizontal osteotomy.19–21 In order to avoid direct nerve injury, the osteotomy should be placed at least 5 mm caudal to the foramen and be executed at a caudal-oblique angle.
Indications and Contraindications
The presence of some medical conditions influences the type of genioplasty that is prudent. Generally, patients with diabetes mellitus or immune deficiency are not ideal candidates for alloplastic augmentation.1,22 Patients over the age of 60 years old with a mild-to-moderate horizontal microgenia are better candidates for alloplastic augmentation. On most other patients osteotomy is preferred, although the use of implants is not considered inappropriate. Patients who smoke cigarettes are not the ideal candidates for the use of grafts as a chin augmentation material.
Preoperative History and Considerations
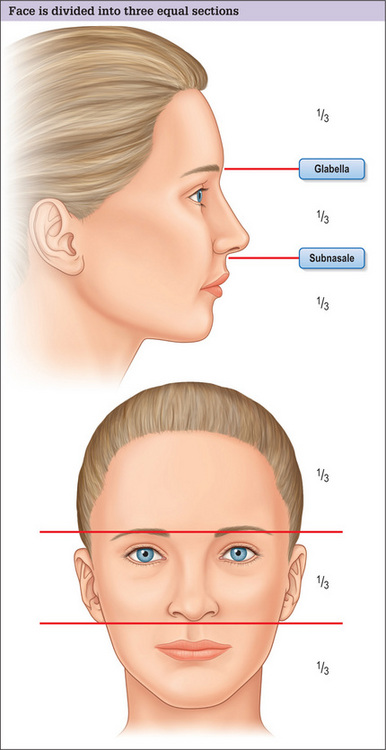
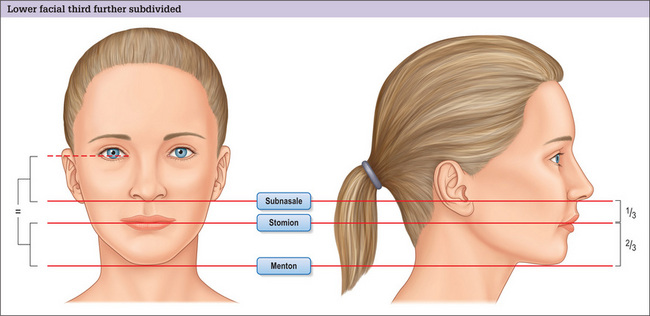
The cardinal determinants of chin harmony are its projection symmetry and vertical length. Assessment of the vertical dimension of the chin is performed first in frontal view analysis. The face is divided into two anatomic portions using imaginary lines placed at the eyebrow level and subnasale. The three segments that these lines create should be equal in the harmonious face (Figs 13.7 & 13.8).
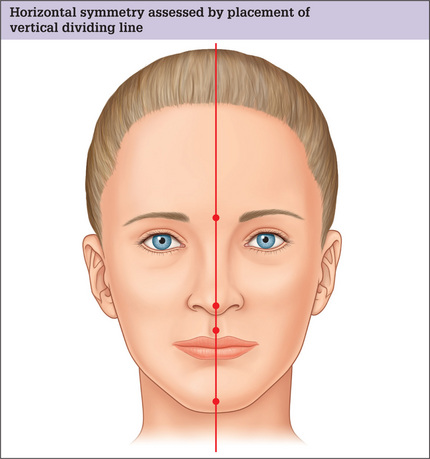
The terminus of the female chin is a single light reflfection. In the male chin, there are dual light reflections indicating the underlying increased width and rectangular shape of the chin. To determine the chin symmetry, a vertical line is drawn passing through the midglabella, the tip of the nose (as long as the nose is straight) and the philtral dimple. The midpoint of a symmetrically located chin will fall on this line (Fig. 13.9).8 If chin asymmetry is identified, its cause should be elucidated as it impacts procedure choice. To decide whether the chin asymmetry is related to maxillary/mandibular disharmony or is intrinsic to the chin itself, the horizontal planes of the mouth and the eyes are examined. The intercommissural line should be parallel to the intercanthal line. Otherwise, vertical asymmetries of one or both of the jaws are likely to be present and genioplasty alone may not correct this condition fully. If the intercommissural line parallels the intercanthal line, a pure genial asymmetry is present and a genioplasty with osteotomy can be planned to correct the deformity (Figs 13.10 & 13.11).
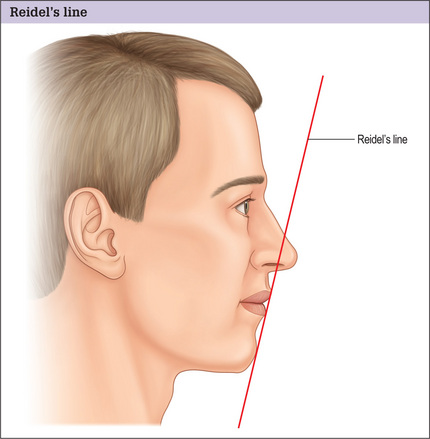
Horizontal excess or deficiency is detected better in profile. There are multiple methods to determine ideal chin projection. The use of Riedel’s plane is simple and practical. With the ideal chin projection present, the most projecting portion of the upper lip, lower lip and chin are all tangent to the same line (Fig. 13.12). If the chin lies posterior to the Riedel’s plane, horizontal microgenia exists. If the chin lies anterior the plane, horizontal macrogenia exists.
An intraoral examination is mandatory in the assessment of the potential genioplasty patient. The maxillary/mandibular occlusal relationship is carefully examined. Significant periodontal disease should be identified and adequately treated prior to genioplasty to decrease the risk of infectious complications.
Life-size photography with soft tissue cephalometric analysis provides an opportunity for precise preoperative planning of augmentation or osseous genioplasty to the millimeter in both the vertical and horizontal planes.23 A circumspect facial analysis, coupled with life-size photography, can lead to an accurate definition of chin dysmorphology.
Classification of Chin Deformity
Chin pathology is classified as types I-VII according to the prevailing boney or soft tissue abnormalities.24 The type of deformity dictates which procedure should be utilized in order to attain a pleasing outcome (Table 13.1).
Table 13.1 Classification of chin deformities
| Group I: Macrogenia |
| Group II: Microgenia |
| Group III: Combined microgenia and macrogenia (bi-planer defects) |
| Group IV: Asymmetric chin |
| Group V: Pseudomacrogenia |
| Group VI: Pseudomicrogenia |
| Group VII: Witch’s chin deformity |
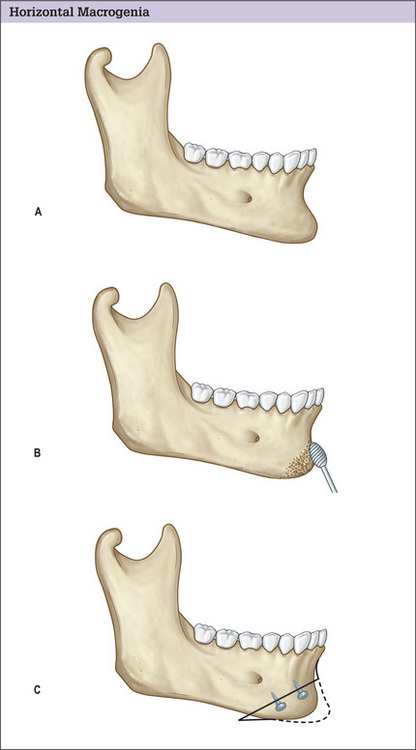
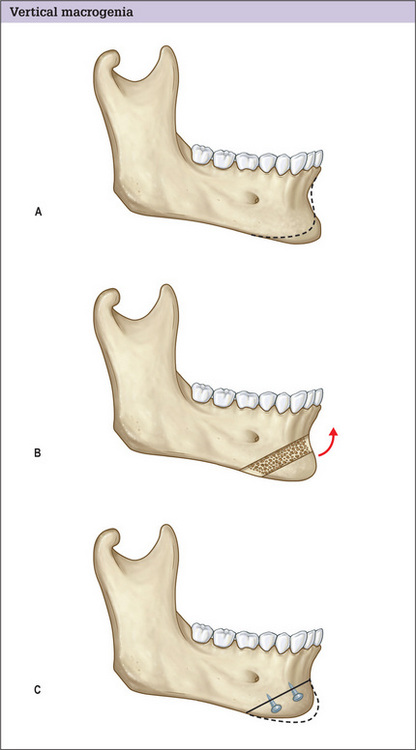
Group I deformities encompass macrogenic chins. Moderateto-severe pure horizontal macrogenia is managed by setting back the caudal segment (Fig. 13.13). Correction of pure vertical chin excess requires resection of a horizontal block or wedge segment (Fig. 13.14).
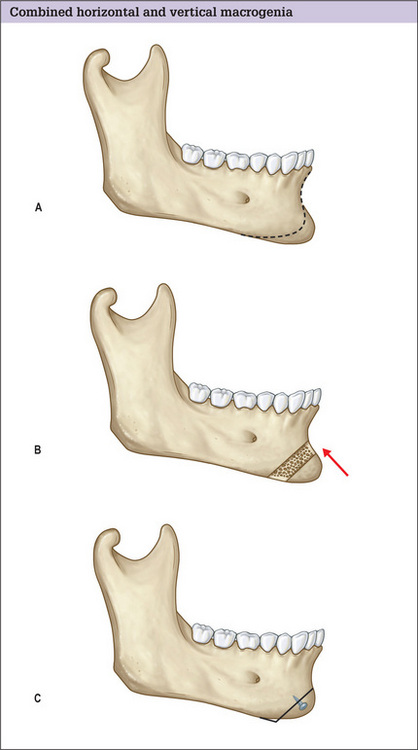
Removal of a horizontal segment with setback of the remaining caudal segment is required for combined horizontal and vertical macrogenia (Fig. 13.15).
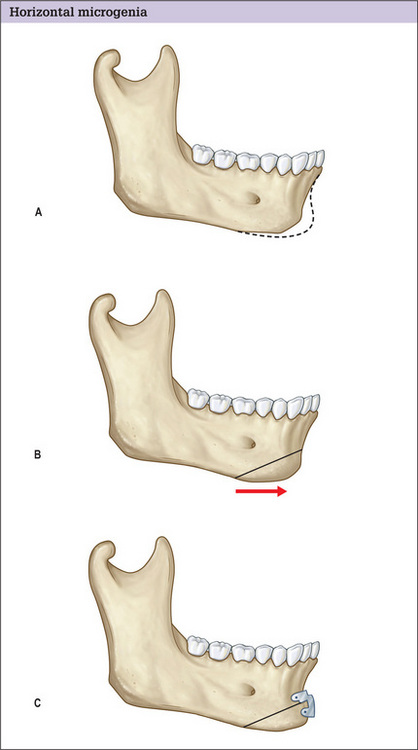
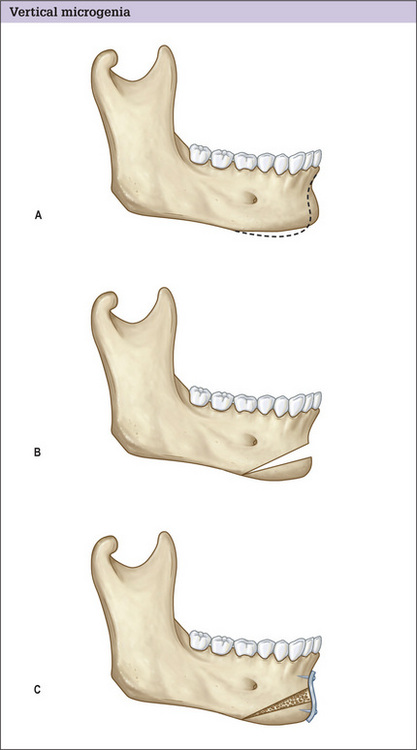
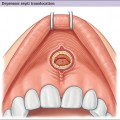
Group II deformities are comprised of microgenic chins. Augmentation genioplasty for mild or even moderate pure horizontal deficiency is discussed in a later section. A horizontal osteotomy with advancement of the caudal segment is a predictable method of treating horizontal chin deficiency (Fig. 13.16). Pure vertical chin deficiency is addressed with a horizontal osteotomy and caudal repositioning (Fig. 13.17). Combined vertical and horizontal microgenia is managed with repositioning the osteotomized chin segment caudally and anteriorly (Fig. 13.18). With any of these osteotomies, whenever caudal repositioning is performed and a gap greater than 5 mm results, interposition bone grafting or placement of a hydroxyapatite block is indicated. Smaller defects are within the osteoblastic filling (jumping) distance.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


