Clinical features
• Chronic plaque psoriasis (most common)
■ Symmetric, well defined red papules and plaques w/ prominent white scale
■ Most common sites: scalp, elbows, knees, presacrum, hands, feet, and genitalia
• Guttate psoriasis: children and adolescents; drop-like lesions measuring 2–6 mm; symmetric distribution; favors trunk and proximal extremities
■ Triggers: group A Strep infection (oropharynx or perianal) or URI (1–3 weeks prior to onset)
• Erythrodermic psoriasis: generalized erythema and scale (>90% BSA)
■ Triggers: poor management decisions most common (e.g., abrupt withdrawal of systemic steroids)
• Generalized pustular psoriasis:
■ Impetigo herpetiformis: pregnancy-associated; begins in flexures then generalizes w/ toxicity; early delivery recommended
■ von Zumbusch: rapid and generalized, painful skin, fever, leukocytosis, hypoalbuminemia, and malaise; a/w hypocalcemia (risk factor)
• Palmoplantar pustulosis: pustules and yellow-brown macules localized to palms/soles; has a chronic course
■ May be a/w sterile inflammatory bone lesions (SAPHO syndrome)
• Acrodermatitis continua of Hallopeau: “lakes of pus” on distal fingers, toes, and nail beds → scale, crust, and nail shedding
■ Scalp: can coexist w/ seborrheic dermatitis; may advance to edge of face, retroauricular areas, and upper neck
○ Psoriasis is #1 cause of pityriasis amiantacea
■ Inverse: shiny pink-red, well-defined thin plaques w/ fissuring
○ Axillae, inguinal crease, intergluteal cleft, inframammary region, and retroauricular folds
■ Oral: annulus migrans (presents like geographic tongue, seen in pustular psoriasis)
■ Nail: fingernails > toenails (vs opposite pattern in onychomycosis)
○ Distal matrix → leukonychia and loss of transparency; subungual hyperkeratosis
○ Nail bed → oil spots, Salmon patches, splinter hemorrhages, onycholysis, and subungual hyperkeratosis
• Psoriatic arthritis (PsA): affects up to 30% of psoriasis patients (correlated w/ skin severity); typically RF-negative (“seronegative”); classic early symptom = morning joint stiffness lasting >1hr; vast majority have nail changes +/− tendon/ligament involvement (enthesopathy/enthesitis); strong genetic predisposition (50% HLA-B27+); Rx: biologics, MTX, apremilast, cyclosporine, and tofacitinib
○ Oligoarthritis w/ swelling and tenosynovitis of hands (60%–70%): affects DIP + PIP joints of hand and feet (may → “sausage digit”) +/− large joint involvement; spares MCP (vs RA)
○ Asymmetric DIP involvement + nail changes (16%): exclusively affects DIP → “sausage digit,” nail damage
○ Rheumatoid arthritis-like (15%): symmetric polyarthritis of small and medium joints (PIP, MCP, wrist, ankle, and elbow); hard to DDx from RA and may be RF+
○ Ankylosing spondylitis (5%): axial arthritis +/− sacroiliac, knee and peripheral joint involvement; M > F, usually HLA-B27+, a/w IBD and uveitis
○ Arthritis mutilans (5%): least common, most severe (osteolysis of phalanges/metacarpals→ short, wide, and soft digits w/ “telescoping phenomenon”)
■ ↓risk of superinfection (due to ↑antimicrobial peptides)
■ ↑risk of cardiovascular diseases, HLD, HTN, DM, NASH, and metabolic syndrome
○ Systemic psoriasis treatments may ↓risk
Histopathology
■ Regular acanthosis w/ elongated rete ridges
■ Thinning of suprapapillary plates
■ ↓ or absent stratum granulosum
■ Dilated capillaries in dermal papillae
■ Micropustules of Kogoj (stratum spinosum) and microabscesses of Munro (stratum corneum)
○ Mnemonic: “Marilyn Munro is always on top (higher in epidermis)”
■ Milder acanthosis, spongiosis, foci of intraepidermal neutrophils, mounded parakeratosis, ↓granular layer
■ Thin, tortuous capillaries in papillary dermis
■ Mixed perivascular infiltrate w/ scattered neutrophils
Treatment
• Topical treatments – may be used alone for mild psoriasis
■ Corticosteroids: first line for mild-moderate psoriasis
■ Vitamin D3 analogs: typically used in conjunction w/ topical corticosteroids
■ Topical retinoids: tazarotene
■ Miscellaneous: salicylic acid, coal tar, and topical calcineurin inhibitors (especially facial and flexural)
• Phototherapy: first line in moderate to severe psoriasis
■ NB-UVB (311–313 nm): highly effective, ↓risk of secondary NMSCs relative to BB-UVB and PUVA
■ BB-UVB: more effective than NB-UVB for guttate psoriasis flares
■ Excimer laser (308 nm): useful for limited/localized disease
■ PUVA: topical for limited areas; oral for more generalized disease
■ Goeckermann regimen: combination of crude coal tar and BB-UVB
• Systemic therapy: moderate-severe psoriasis
■ Apremilast (PDE-4 inhibitor), tofacitinib (JAK 1/3 inhibitor) = newest oral agents for psoriasis
■ Cyclosporine: do not use >1yr; ↑risk SCCs (particularly in a/w PUVA)
■ Systemic retinoids: acitretin is the only systemic retinoid used in psoriasis; monotherapy effective in erythrodermic and pustular psoriasis; combination w/ phototherapy (Re-PUVA) effective for plaque psoriasis
○ TNF-α inhibitors: infliximab, etanercept, and adalimumab
○ IL-12 and IL-23 inhibitor: ustekinumab
○ IL-17 inhibitors: secukinumab (FDA approved in 2015), brodalimumab, and ixekizumab (FDA approved in 2016)
Additional boards factoids
• Woronoff ring: pale blanching ring around psoriatic lesions
• Auspitz sign: scraping of psoriasis scale → pinpoint bleeding (due to dilated capillaries and suprapapillary plate thinning)
■ Pustular (von Zumbusch): acitretin (>cyclosporine, MTX, and biologics)
■ Impetigo herpetiformis: early delivery, prednisone
■ Guttate: BB-UVB at erythemogenic doses (>NB-UVB)
Pityriasis rubra pilaris (PRP)
Clinical features
• Classically begins on head/neck → progresses caudally
■ Scalp erythema w/ fine, diffuse scaling
■ Folliculocentric keratotic papules on erythematous base (“nutmeg-grater” papules)
○ Papules coalesce into orange to salmon-colored plaques w/ “islands of sparing” on trunk and extremities → can progress to erythroderma w/ exfoliation
■ Orange-red waxy keratoderma of palms/soles (“sandal-like PPK”) w/ fissures
■ Thick, yellow-brown nails w/ subungual debris; lacks nail pits (vs Pso)!
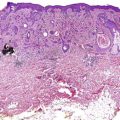
• Five distinct subtypes (Fig. 3-2) and a sixth newer subtype (generalized PRP in HIV patients w/ hidradenitis suppurativa, acne conglobata, and elongated follicular spines); all except type 4 are generalized
■ Type 1 (55%, classic adult): most common form, rapid onset of classic PRP features, good prognosis (80% resolve within 3 yrs)
■ Type 2 (5%, atypical adult): slow onset, ichthyosiform leg lesions + keratoderma w/ coarse and lamellated scale +/− alopecia; chronic course
■ Type 3 (10%, classic juvenile): same presentation/course as type 1; peaks in adolescence and first 2 yrs of life
■ Type 4 (25%, circumscribed juvenile): most common form in children (Fig. 3-3); only localized form of PRP; p/w follicular papules and erythema on elbows and knees; prepubertal onset; variable course
■ Type 5 (5%, atypical juvenile): first few years of life, PRP + sclerodermoid changes of hands/feet; chronic

Histopathology
• Alternating vertical and horizontal orthohyper- and parakeratosis (“checkerboard pattern”)
• “Shoulder parakeratosis” (parakeratosis at edges of hair follicle orifice)
• Irregular acanthosis w/ thickened suprapapillary plates (vs Pso)
• Focal acantholysis or acantholytic dyskeratosis (recently-appreciated findings)
Seborrheic dermatitis
Clinical features
■ Erythematous, scaly, sometimes pruritic rash affecting “seborrheic” areas (scalp, face, postauricular, presternal, and intertriginous areas)
■ Infants often present w/ “cradle cap” (greasy yellow scales adherent to scalp)
■ Erythematous, scaly, macerated plaques in body creases (anterior neck crease, axillae, groin, and popliteal fossae)
■ Well-defined, pink-yellow patches w/ “greasy” scale in highly sebaceous areas (scalp, eyebrows, nasolabial folds, forehead, ears/retroauricular, central chest, and intertriginous areas)
■ Often itchy (particularly scalp)
■ Dandruff (pityriasis simplex capillitii) – mild form on scalp
Pityriasis rosea (PR)
Clinical features
• Begins w/ “herald patch” = solitary pink, enlarging plaque w/ fine central scale and larger trailing collarette of scale; favors trunk
• Diffuse eruption (begins hours to weeks later): oval patches/plaques on trunk and proximal extremities
■ Lesions appear similar to “herald patch,” but smaller
■ Vertical axes oriented along Langer’s lines (“Christmas tree pattern”)
■ 25% experience significant pruritus
• Atypical pityriasis rosea: term utilized when rash has unusual features, including:
■ Inverse PR pattern: prominent involvement of intertriginous sites, or more prominent involvement of limbs (> trunk)
■ Papular, vesicular, or targetoid morphology
○ PR is often more papular and extensive in African American children
■ Oral involvement (e.g., ulceration)
• Drug-induced PR-like eruptions: ↑inflammation/pruritus, lacks herald patch; older patient population
Intertriginous/axillary granular parakeratosis
• Adult women > infants (diaper area)
• Pruritic, keratotic red-brown papules and plaques in intertriginous areas (axillae > inguinal, inframammary)
• Possible defect in filaggrin metabolism → retention of keratohyaline granules in SC
■ Alternative theories: irritant dermatitis, reaction to deodorants/antiperspirants
• Histology: characteristic thickened eosinophilic stratum corneum w/ prominent parakeratosis and retained keratohyalin granules; vascular ectasia (Fig. 3-4)
• Rx: topical (corticosteroids, vitamin D analogues, keratolytics, and antifungals), destructive (cryotherapy), and systemic (isotretinoin, antifungals)
Erythroderma
Clinical features
• Erythema and scale involving >90% of BSA
• Not a defined entity, but rather a clinical presentation of various disorders, characterized by:
■ Pruritus (>90% of cases, especially atopic dermatitis or Sezary); lichenification (>30%); dyspigmentation (>50%); PPK (30%); nail changes (40%, typically “shiny nails”)
■ Other skin findings: S. aureus colonization, eruptive SKs, ectropion, and conjunctivitis
■ Systemic findings: peripheral lymphadenopathy (#1 extracutaneous finding), hepatomegaly (20%), pedal/pretibial edema (50%), tachycardia (40%), thermoregulatory disturbances (hyperthermia > hypothermia), hypermetabolism, and anemia
• Primary (erythema involves whole skin surface in days to weeks) vs secondary (generalization of localized skin disease)
■ Psoriasis (most common cause in healthy patients):
○ Usually preceded by typical plaques
○ 25% are idiopathic; less scaly than typical psoriasis lesions
○ Erythroderma is usually due to drug withdrawal (steroid, MTX, or CSA)
○ Nails w/ characteristic psoriasis findings
○ Histologically, changes of early psoriasis seen
○ Typically have atopic history
○ Severe pruritus and lichenification
○ Most common cause in HIV patients (40% vs 23% in non-HIV patients)
○ Lesions may become purpuric in ankles and feet
○ Shorter duration than other erythrodermas (resolves 2 to 6 weeks after drug withdrawal)
○ Most common drugs: allopurinol, sulfa (TMP-SMX, dapsone), antiepileptics, INH, minocycline, and HAART
■ Idiopathic erythroderma: elderly men w/ relapsing course
○ Lymphadenopathy, PPK, and peripheral edema seen frequently
■ CTCL (Sezary and erythrodermic MF):
○ Sezary: primary erythroderma; T-cell clone in blood plus one of the following: 1) ≥ 1000 Sezary cells/µL; 2) CD4:CD8 ratio of ≥ 10 : 1; or 3) ↑percentage of CD4+ cells w/ abnormal phenotype (loss of CD7 or CD26)
○ Erythrodermic MF: secondary erythroderma; due to progression from classic MF patches/plaques
■ Less common causes: PRP, GVHD, paraneoplastic erythroderma, bullous dermatoses, and ichthyoses
Confluent and reticulated papillomatosis (CARP)
• Starts at puberty; F > M; blacks > whites
• Red or brown, rough, keratotic, slightly raised papules that first appear in intermammary region → spreads outward and forms reticulated pattern (Fig. 3-5) laterally

• Histology: acanthosis nigricans-like (hyperkeratosis, acanthosis, and papillomatosis)
• ToC: Minocycline 100 mg BID x 6 weeks (effective in 50%)
• Other options: oral retinoids, oral antibiotics, or topical antifungals
• Pseudoatrophoderma colli: variant that occurs on neck; appears as vertically-oriented hyperpigmented papillomatous lesions w/ wrinkling; also responsive to minocycline
3.2 Eczematous dermatoses
Atopic dermatitis (AD)
Epidemiology
• Part of atopic triad: AD (often first manifestation), allergic rhinitis, and asthma
• More common in high income and urban areas (exposure to pollutants and lack of exposure to infectious agents may trigger development of AD)
• Affects 25% of children, 3% of adults
■ Early onset (most common): arises by 1–2 yo, 50% have allergen-specific IgE antibodies, 60% resolve by 12 yo
■ Late onset: arises after puberty
■ Senile onset: arises after 60 yo
• Onset: 50%–60% by first year of life (often 3–6 months), 90%–95% by 5 yo
Pathogenesis
• Complex interaction of epidermal barrier dysfunction, immune dysregulation, and environment
• Genetic factors are important
■ Twin studies (monozygotic > dizygotic concordance) and family history (high probability that one or both parents are atopic)
■ Genes encoding epidermal proteins (e.g., FLG and SPINK)
○ Filaggrin (FLG) mutations cause alterations in epidermal barrier; strongly a/w AD development, especially severe early onset AD
○ Barrier dysfunction causes transepidermal water loss and xerosis, allowing penetration of allergens
■ ↑transcription of genes encoding immunologic proteins (TLR2, FCER1A, and DEFB1) and cytokines (Th2 > Th1 cytokines involved in regulation of IgE (especially IL-4, IL-5, IL-12, and IL-13))
○ Acute AD: Th2 predominance w/ eosinophilia, ↑IgE production and ↓cutaneous antimicrobial peptides
○ Chronic AD: Th1 predominance w/ ↑IFN-γ
■ Histamines less important than neuropeptides, proteases, kinins, and certain cytokines
Clinical features
■ Plus ≥ three of the following:
○ Personal history of allergic rhinitis or asthma
○ History of skin crease involvement (antecubital, popliteal, ankle, neck, and periorbital)
• Acute form: erythema, edema, vesicles, oozing, and crusting
• Subacute and chronic forms: lichenification, papules, nodules, and excoriations
■ Infantile (birth to 6 months of age)
○ Acute presentation and clinical features
○ Favors face, scalp, and extensor surfaces
○ May have overlap with seborrheic dermatitis
○ Clinical manifestations typically more chronic in nature, though acute flares may occur
○ Diffuse xerosis becomes more prominent
• Adolescent/adult AD (>12 yo)
■ Lichenified plaques > weeping eczematous lesions
■ Prominent involvement of flexures, face, neck (retroauricular) upper arms, back, and acral sites
■ AD beginning during childhood is a/w more severe, treatment-resistant disease as in adults
■ May manifest as isolated prurigo nodularis, hand or eyelid dermatitis
• Senile AD: marked xerosis rather than typical AD lesions
■ Triggers: wool clothing, sweat, and stress
• Associated features of AD: xerosis, ichthyosis vulgaris, keratosis pilaris, palmoplantar hyperlinearity, Dennie-Morgan lines, periorbital darkening, circumoral pallor, anterior neck folds, Hertoghe sign (diminished lateral eyebrows), white dermatographism, follicular prominence (favors darker skin types), “allergic shiners” (grey infraorbital discoloration), and exaggerated linear nasal crease (“allergic salute”)
■ Children have ↑incidence of: pityriasis alba (hypopigmentation seen on face/neck; more common in darker skin types and more visible after sun exposure), lichen spinulosis, nummular dermatitis, dyshidrotic eczema, and juvenile plantar dermatosis
• Infectious complications: secondary to impaired barrier function and immunologic factors
■ Bacterial: impetiginization w/ S. aureus > S. pyogenes
■ Viral: eczema herpeticum, molluscum dermatitis, and eczema vaccinatum (seen w/ smallpox vaccination)
• Ocular complications: atopic keratoconjunctivitis (adults), vernal keratoconjunctivitis (children, warm climates), posterior subcapsular cataracts, keratoconus (elongation of the cornea), and retinal detachment
Regional variants
• Ear: erythema/scaling/fissuring under earlobe and retroauricular region
• Eyelid: lichenification of periorbital skin
• Frictional lichenoid eruption: occurs during spring and summer in boys on elbows/knees/dorsal hands (clusters of small 1–2 mm lichenoid papules)
• Hand: may be intrinsic (atopic, psoriasis, dyshidrotic, hyperkeratotic), extrinsic (irritant or water exposure, or allergic), or infectious (tinea, S. aureus) in nature
■ Dyshidrotic eczema on lateral fingers and palms: “tapioca-like,” firm and deep-seated pruritic vesicles
○ Pathogenesis is multifactorial (irritant, atopic, and allergic contact)
○ Often chronic and recurrent/relapsing
• Diaper (napkin dermatitis; please refer to Pediatric Dermatology chapter)
• Id reactions (autosensitization)
■ Classic example: a vesicular eczematous id reaction of the hands arising in a pt w/ tinea pedis; secondary id reaction resolves when underlying dermatosis is treated
• Juvenile plantar dermatosis (please refer to Pediatric Dermatology chapter)
• Lip (cheilitis sicca): irritant contact dermatitis (including “lip-licker’s eczema”) > allergic contact dermatitis (fragrance mix most commonly) > atopic dermatitis > eczema of unknown cause
■ Worse in winter; vermilion lip most affected
• Head and neck: occurs post-puberty, Malassezia may aggravate
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


