Daily walking stance benefits the health, whereas lower extremity reconstruction aims to accomplish balanced walking and posture control. If local flap or tendon transfer cannot provide the basic function, microsurgical reconstruction is indicated for bony, soft tissue, and sensation restoration. Wound repair can use every modality and can achieve varying wound coverage results. However, all reconstruction should have functional goals using either local flap or free flap to restore the lost function. With less recipient site secondary damage, microsurgery can provide healthy composite tissue with like-replaces-like approach to create more stable long-term results.
Key points
- •
All reconstruction should have functional goals using either local flap or free flap to restore the lost function.
- •
If local flap or tendon transfer cannot provide the basic function, microsurgical reconstruction is indicated for bony, soft tissue, and sensation restoration.
- •
Major functional unit rebuilding is the goal for jeopardized function in lower limbs.
- •
Free tissue transfer can have the advantage of composite tissue inclusion and spatial arrangement using the fascial component for tendon or muscle defect reconstruction.
Introduction
Various trauma or tumor surgery on lower limbs can result in not only soft tissue envelope defects but also variable functional deficits. Numerous resurfacing procedures are available to repair the defects. Improvements in sterile technique, the use of antibiotics, bony fixation, and microvascular reconstruction have shifted the management paradigm of mutilating limb and limb salvage to functional restoration. The ultimate goal of reconstructing a lower extremity is to achieve painless, stable weight-bearing walking, which requires adequate bone union, a pliable stable joint, and a sensate sole.
In the scenario of open wounds, all the vital structural defects can be well recognized and assessed, and the required recipient neurovasculature is exposed entirely. It is best to plan either a 1-stage or staged reconstructive strategy. Severely contaminated or mutilated limbs make the viability of the traumatized tissue questionable, so the lesion may require repeated debridement before the coverage reconstruction. If the wound infection or contamination is under control, functional reconstruction can be combined with the resurfacing procedure to provide a simultaneous soft tissue and functional restoration.
The authors believe that functional reconstruction should incorporate conventional or microsurgical methods for the restoration of functional loss. Methods such as vascularized bone transfer, bone grafting or distraction, tendon transfer, free functioning muscle transfer, and sensate glabrous skin for plantar defect resurfacing are all designed for functional considerations.
The restoration of a stable, strong femur or tibial bony structure is essential for weight bearing. Conventional bone graft or bone substitute can be used for small-segment bony defects.
Improvements in microsurgical free tissue outcomes contribute to the functional result and quality of life. Establishment of comprehensive wound repair, bony union, and motor unit transplant is the standard for adequate lower extremity functional restoration.
Despite the psychological advantages of limb salvage, the return to premorbid status is equivalent to limb amputation. Thus the reconstructive procedures should be designed to accomplish comprehensive coverage and functional management to shorten the disability and return to work times.
Indications and contraindications of preferred reconstructions, including rationale and timing
The Lower Extremity Assessment Project (LEAP), the first and only prospective, multi-institutional cohort study of several scoring systems on severe lower extremity trauma, found no association between loss of plantar sensation and the need for late amputation, dispelling one of the classic absolute indications for amputation. A comparison of functional outcomes between the amputated and salvaged cohorts found no significant differences.
The scores are not definitely compatible with the functional outcomes. Even low scores tend to have higher lower limb salvage rate. Many patients with high scores have successful salvage or functional outcomes. Recontracture surgery is not appropriate for reconstructable limbs. , Thus, reconstructable limbs are related to the facility of the hospital or collaborative team. Appropriate referral of the traumatized patients to a competent team at the right time is essential.
However, before the definite reconstruction, all patient should have justified damaged control for the polytrauma insult. Particularly in patients presenting with impending lethal triad, the overwhelming pathophysiologic effect of severe inflammatory response syndrome or complementary antiinflammatory response syndrome can be life threatening.
In recent decades, free tissue transfers, local flaps, or pedicle perforator flaps have been widely used for posttraumatic lower limb defect reconstruction. Resurfacing surgeries aim at wound repair, either skin, muscle, or osteocutaneous flaps. To go a step further, functional restoration can enhance the benefit for functional deficits of lower limbs. Simultaneous or secondary tendon transfer, or arthrodesis, is applied for functional purposes. Composite free tissue can comprise different components to improve the functional unit loss in various reconstructions.
Established Principles and Surgical Approaches
Beyond the resurfacing procedure, there are several functional deficits that benefit from free tissue transfer or microsurgery, including (1) bony structure rebuilding to allow weight bearing; (2) contracture release of knee, ankle, or toe joints; (3) muscle or tendon defects; (4) denervation; and (5) durable weight-bearing soles.
- 1.
Bony structure rebuilding to allow weight bearing
Conventional bone grafting is feasible for small bone defects in well-vascularized recipient sites. Vascularized bone flap transfer is indicated for unfavorable situations and Illizarov bone transportation is another alternative. Vascularized bone flap is preferable for (1) segmental bone defects >6 cm with/without soft tissue defect, (2) chronic osteomyelitis, (3) pseudoarthrosis, (4) multiple failure in conventional bone grafting, and (5) poor vascularity of recipient site. There are many donor bone flaps that fit the mentioned indications, such as fibula, iliac crest, and rib flap. Fibular flap possesses more cortical bone strength, constant blood supply, and less donor site morbidity. Stress fracture is common after bone flap transfer, thus protective brace and crutch walking should be applied for both internal fixation or temporary external fixator removal until there is adequate bony hypertrophy. The double-barrel fibular flap can also provide more area and volume in cross section for long bone defects. Therefore, fibular flap is the first option for long bone reconstruction.
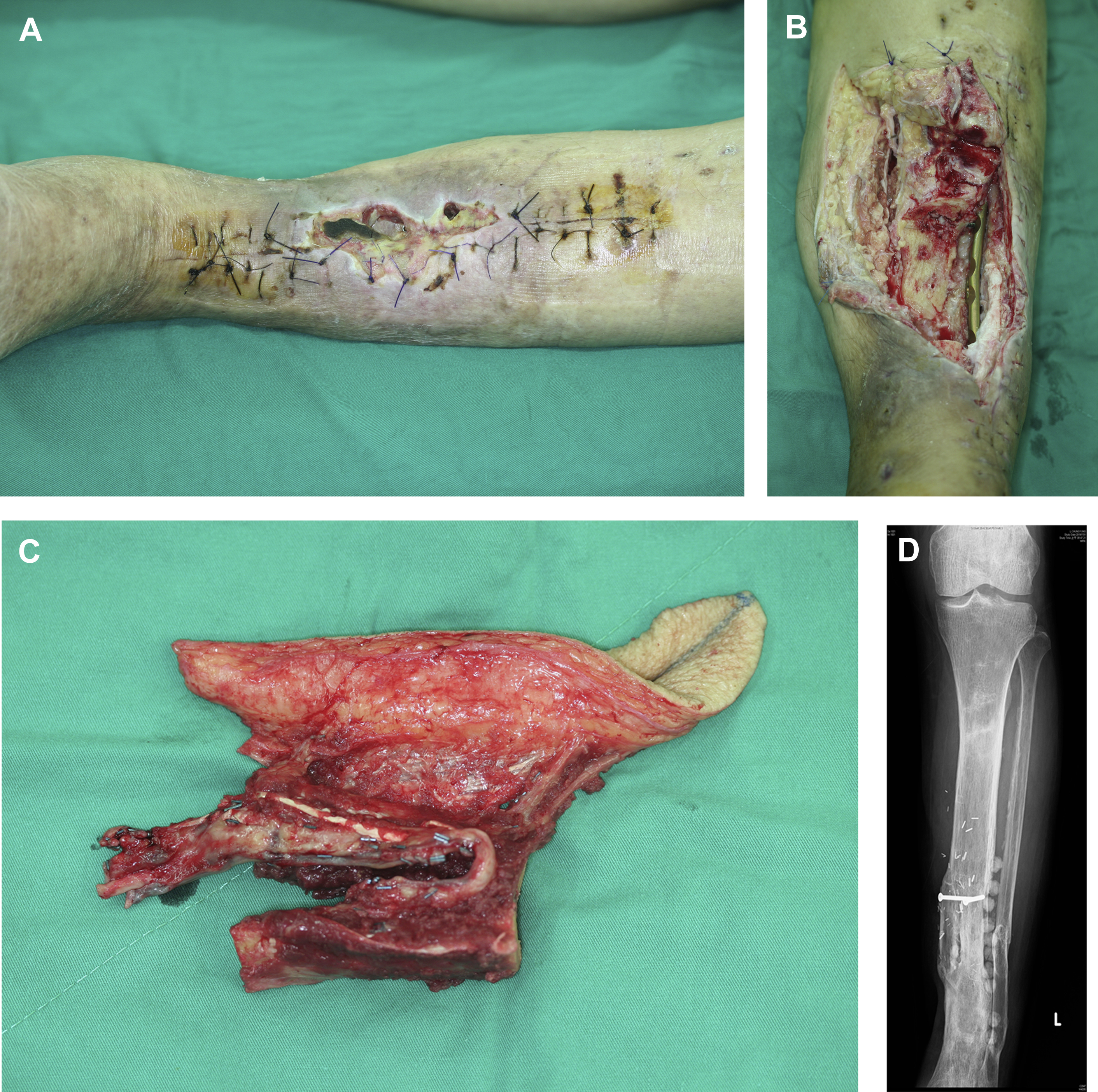
The functional purpose is to have bony union, adequate bone hypertrophy, and full weight bearing within 2 years with the least chronic osteomyelitis and stress fracture ( Fig. 1 ). Comparing the donor site and recipient morbidity, and the functional outcomes among the fibular flap, iliac flap, and rib flap, the fibular flap was the best for lower extremity bony reconstruction, which can be performed as a double barrel for the volume augmentation to increase the strength for weight loading and less stress fracture( Fig. 2 ). Iliac flap can have good bony union, but less hypertrophy, and limited bony length is available. The serratus anterior combined rib flap is a membranous bone that is thin and requires a lengthy time for bone hypertrophy and consolidation, but, with the accompanying latissimus dorsi muscle based on the thoracodorsal pedicle, this composite flap can reconstruct extensive defects. In bilateral tibiofibular open IIIB fractures, the serratus anterior-rib flap can be an alternative method to rebuild the bilateral lower limb composite defect ( Fig. 3 ).
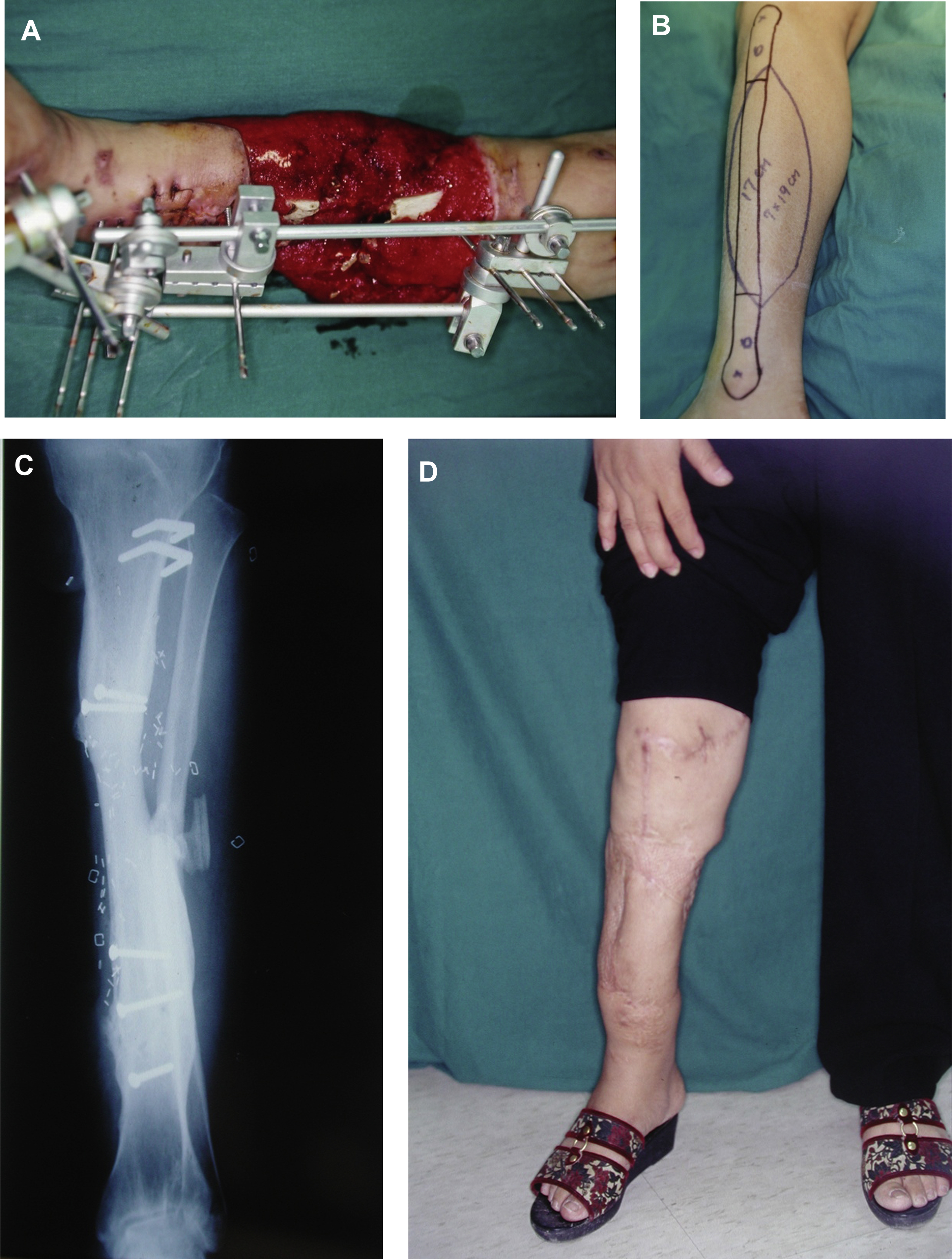
Fig. 1
( A ) This female patient in her 40s sustained right tibial open IIIB fracture with composite defect. ( B ) Fibular osteocutaneous flap. ( C ) Advanced bony hypertrophy. ( D ) Eight-year follow-up.
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


