Proper hand function relies on a combination of strength and mobility. The intricate architecture that allows for hand mobility includes the articular surfaces of joints, periarticular ligamentous structures, tendon mechanisms, and the soft-tissue envelope. These structures are subject to injury and scarring. The net effect of a variety of etiologic factors is stiffness of the hand with diminution of hand function. This article reviews the biology of healing, pertinent anatomy of the hand, and operative and nonoperative treatment of the stiff hand.
Proper hand function relies on a unique combination of strength, stability, discriminate sensation, and mobility. Disruption of this delicate balance results in diminution of hand function and loss of the ability to perform not only fine tasks but also basic activities of daily living. Joint contracture and stiffness of the hand are the net effect of several underlying etiologic factors including congenital abnormalities, neurologic disease, traumatic injury, prolonged immobilization, arthritis, and regional pain syndromes. These etiologic elements are often interrelated and multifactorial. Stiffness of the hand represents a challenging problem for surgeons and therapists, and remains the key impediment to achieving desired surgical outcomes in joint and soft-tissue reconstruction of the hand including tendon repair, replantation, and joint arthroplasty.
Evaluation and treatment of the stiff hand requires application of a systematic approach that integrates an understanding of the mechanism of injury, anatomic structures involved, and the modalities and proper timing of treatment available. Successful management relies on a cooperative effort, integrating the expertise of hand surgeons and therapists with patient education and diligence. This article provides an overview of the etiology, evaluation, and treatment of the stiff joint.
Etiology of joint stiffness
Wound Healing and Scar Formation
Joint motion is reliant on a balance between the rigid bony and ligamentous structures and the supple gliding of the joint surface, tendons, and the overlying soft tissues. Following a traumatic injury, infection, or surgical procedure, a predictable cascade of events is set in motion that seeks to restore tissue integrity. Although intricate, this wound-healing cascade cannot perfectly replicate or replace the damaged structures of the hand; rather, bone, tendon, synovium, and skin are replaced with callous and scar. An understanding of this wound-healing progression provides a framework for the application a variety of treatment modalities including splinting, mobilization, and operative intervention.
Wound healing comprises 3 overlapping phases: inflammatory, proliferative, and remodeling or maturation. The inflammatory phase begins with vascular disruption and the exposure of subintimal collagen. This insult leads to the activation of both the clotting and complement cascades. Cytokines and chemokines released from platelets and neutrophils trigger vascular dilation, increased vascular permeability, and cell migration to the region of injury. Increased capillary permeability allows for protein-rich exudate to accumulate within the interstitial space. Coupled with decreased lymphatic outflow, this increased permeability results in localized edema and is itself a primary contributor to stiffness. Edema results in direct, hydrostatic joint capsular distension and resistance to the normal gliding movements of the joints and tendons throughout the hand. If chronic, interstitial edema may become fibrotic as the fibrinogen-rich exudate is converted into interstitial scar, resulting in direct adhesion between normally mobile tissues.
Inflammatory leukocytes (neutrophils and macrophages) are recruited to the site of injury. These cells produce matrix metalloproteinase enzymes that act to degrade extracellular matrix components, clearing necrotic debris and laying the foundation for fibroblast-dependent collagen synthesis and subsequent scar formation. This second, proliferative phase is marked by the synthesis of disorganized type III collagen, and angiogenesis. Collagen is deposited along the joint capsule and collateral ligaments as well as along the flexor and extensor tendons. Wound healing progresses from the proliferative phase to the third phase of wound maturation and remodeling. Scar maturation is characterized by breakdown of the disorganized type III collagen and replacement with highly organized, cross-linked type I collagen. This scar is indiscriminate, providing necessary strength while obliterating the normal anatomic architecture and distinct tissue planes that facilitate joint motion. Scar maturation is also characterized by scar contracture or tightening as a direct result of myofibroblast activity. The net effect is one of distorted anatomic structures, destruction of normal anatomic planes, and the direct connection of typically mobile structures to fixed ones.
Articular, Periarticular, and Tendon Anatomy
Alterations in the articular surface, periarticular ligamentous structures, and the flexor and extensor tendon mechanisms act alone or in concert to contribute to joint stiffness. Joint surfaces within the hand are analogous to larger articular surfaces found throughout the body. These surfaces are characterized by smooth yet durable articular cartilage with an intervening synovial space. Loss of this architecture through mechanical degradation in the form of osteoarthritis or secondary to traumatic events including intra-articular fractures can lead to deterioration in joint mobility. Intra-articular anatomy is closely aligned with periarticular structures that provide stability about the joint. These periarticular structures are highly specialized in the hand, and deserve particular attention when considering the etiology of joint stiffness.
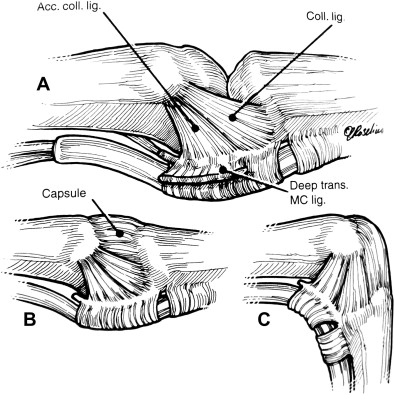
The metacarpophalangeal (MCP) joint is a multiaxial condyloid joint. Motion about this joint includes flexion, extension, abduction, adduction, and a limited degree of circumduction. The joint is stabilized by a taut volar plate that serves to prevent hyperextension, and a redundant dorsal capsule that allows for full flexion. Collateral and accessory collateral ligaments are present on the radial and ulnar sides of the joint coursing from metacarpal head to the base of the proximal phalanx in a dorsal to volar direction. These ligaments stabilize the joint against radially and ulnarly directed forces ( Fig. 1 ). The consequence of this tangential orientation is that the collateral ligaments and capsule are taut with the MCP joint in flexion. This position also minimizes the intra-articular volume. Edema in the setting of inflammation about the MCP joint has a tendency to force the joint into extension, maximizing intra-articular volume and placing the collateral ligaments in a position of laxity. If this position persists throughout the phases of wound healing, the MCP joint will become stiff in this position of extension, with shortened collateral and accessory collateral ligaments.