14 Frontalis and HFL
Summary and Key Features
• Botulinum toxin can be safely utilized to treat horizontal forehead lines
• Most adverse effects resulting from the cosmetic use of botulinum toxin resolve spontaneously
• The risk of adverse outcomes after forehead treatment is increased by certain predisposing factors: age greater than 50 years, mild brow ptosis at baseline, pre-existing low eyelid platforms, and dermatochalasis
• Individualized injection techniques are recommended for individuals with tall (wide) and short (narrow) foreheads
• The frontalis muscle is very responsive to treatment and therefore low doses of toxin should be utilized initially
• Botulinum toxin (given around the time of suturing) has also been shown to be effective for minimizing the appearance of scars due to surgical and traumatic wounds
Side effects
Potential side effects from botulinum toxin use in the forehead include injection site pain, swelling, and bruising, as well as headache, eyebrow ptosis, eyelid ptosis, diplopia, and the development of new rhytides. New rhytides may appear as a result of overcompensation of untreated adjacent muscles. A case series by Kang et al (2011) of four patients receiving BoNT-A for HFLs reported the development of lower frontalis and glabellar protrusions as well as new unilateral forehead rhytides above the eyebrow. In all patients, most of the new rhytides were almost completely resolved within 4 weeks without further treatment. Indeed, the majority of side effects resulting from cosmetic use of botulinum toxin in the forehead as well as in other aesthetic regions resolve spontaneously without treatment.
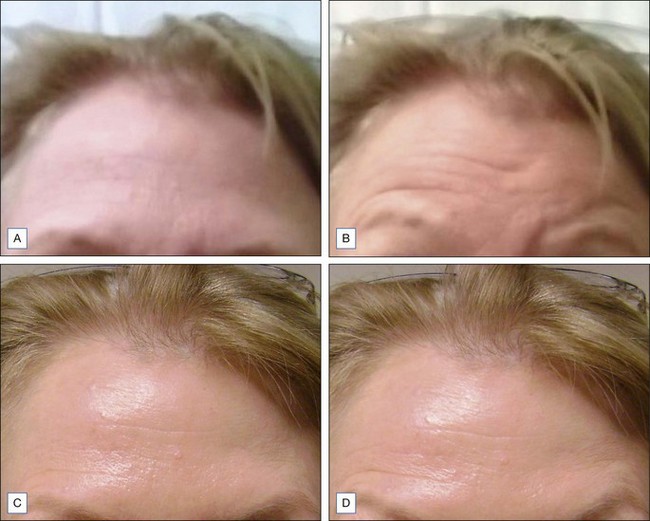
Other possible side effects from botulinum toxin treatment of HFLs include eyebrow and eyelid ptosis and periorbital edema, which are also self-limited. BoNT-A agents have been shown to spread up to 3 cm from the site of injection, but this may depend on the actual agent used and the method of dilution. Certain predisposing factors for eyebrow ptosis include age greater than 50 years and patients with mild eyebrow ptosis at baseline. Patients with pre-existing low eyelid platforms (i.e. the upper eyelid itself hangs down to or near the level of eyelashes) and dermatochalasis (Fig. 14.1; redundant skin at the eyebrow that hangs down toward the eyelid) should also be carefully evaluated to decide whether or not to proceed with treatment of the HFLs. Techniques that may help to prevent eyebrow ptosis include simultaneous treatment of brow depressors (especially the superior–lateral aspect of the orbicularis oculi) and to avoid eyelid ptosis by choosing injection points sufficiently superior to the orbital rim.