The freestyle local perforator flap is an advanced version of the conventional island pedicle flap. Intramuscular dissection can provide a longer pedicle, which allows restoration of defects that are future from the donor site. Without microsurgery, the flap can be either rotated or advanced toward the defect, making it particularly useful for reconstructing soft tissue defects in the lower third of the leg. Careful preoperative design with vessel mapping, skillful intramuscular dissection of the pedicle, and a well-considered backup plan in case of unexpected difficulty are crucial for freestyle local perforator flaps to be successful.
Key points
- •
The freestyle pedicled perforator flap is an advanced version of the island pedicle flap that can be elevated from various parts of the body to cover soft tissue defects.
- •
Intramuscular dissection can provide a longer pedicle and reach defects more easily.
- •
Precise preoperative planning and design, including a backup plan, are essential for the success of free style local perforator flaps.
- •
Careful patient selection allows for optimal reconstructive outcome with minimal donor site morbidity.
Introduction
The reconstructive choice of skin coverage and soft tissue defect in the lower leg depends mainly on its location and extent. In the past half century, the gastrocnemius and soleus muscle flaps have been commonly used for upper and middle third defects, but the lower third has to undergo microsurgical free flap transfer, because of the lack of both local muscle and skin flaps with adequate vascular pedicle length.
Conventionally, the vascular pedicle of a pedicled skin island flap depends only on the presence of a direct or a septal vessel that is, the terminal branch of a source vessel or a branch arising from a source vessel and running between muscles before reaching the skin. However, there is a third type skin vessel, probably the most common one, known as the “myocutaneous perforator,” which has an intramuscular course between its source artery and its entry to the skin. Pedicled island flaps that depend on this type of skin vessels were often not useable in the past because of their limited pedicle length, which did not allow the flap to reach far enough to lower third defects in the leg. However, in the middle of 1990s, intramuscular dissection of the “myocutaneous perforator” from its surrounding muscle fibers became possible. The flap elevated using this technique, was named “perforator flap” by Koshima and Soeda. Perforator flaps have since then revolutionized reconstruction from free skin flaps to “perforator”-based flaps. This development was made possible by the angiosome theory of Taylor and Palmer and uses Doppler probes for vascular mapping on skin flaps.
Initially, the perforator flap was mostly harvested as a microsurgical free flap. Rapid accumulation of experience from pioneers, , as well as better understanding of the vascular territory of individual vessels, intervessel connections, and perfusion characteristics of each clinically significant perforator, led to revisits of many donor sites previously considered unusable for harvesting a cutaneous flap. It was found that, when intramuscular dissection is done, the pedicle becomes long enough that such flaps could indeed be raised. Hence, reconstructive microsurgery entered a new era of perforator flaps. In 1983, Asko-Seljavaara introduced the concept of “freestyle free flap,” which was subsequently materialized by Wei and Mardini and Feng and colleagues with several clinical series. Many small to moderate dimensioned skin flaps could be harvested from previously unknown areas, as long as the supplying vessel can be identified. The same principle is applicable to many local island skin flaps traditionally considered nonfeasible, particularly for small and moderate defect coverage.
This article focuses on local perforator-based island skin flaps and their indications, contraindications, and preoperative preparations, including vascular mapping, flap selection and design, and flap dissection techniques. Various types of flap transpositions were shown with clinical cases.
Indications and contraindications
Indications for freestyle local flap for lower leg reconstruction include the following:
- 1.
Small to moderate size defects of the lower leg.
- 2.
Defects require like-with-like reconstruction, where local or regional flaps provide a superior aesthetic and functional match.
- 3.
Raising a flap with anatomic anomalies, including no sizable perforators found during the dissection.
- 4.
Patients who have undergone multiple flap procedures that have exhausted the typical donor sites.
- 5.
Revision of previously transferred flap with difficult second or sequential reconstruction.
Contraindications
- 1.
Personal history of heavy smoking.
- 2.
Extended trauma or profound infection of lower extremity
- 3.
Previous radiotherapy around the defect.
- 4.
Nonsizable perforator found during the dissection.
Preoperative evaluation and special considerations
Freestyle flaps can be harvested from any location where a skin vessel is found. Defect-related parameters and donor site considerations can assist flap selection. The donor sites can be selected based on the “ideal” flap theory. Suitable freestyle flaps for lower leg reconstruction ideally meet following criteria: versatility in design, adequate tissue volume, good texture and color match, reliable large and long pedicle, straightforward flap dissection, and minimal donor site morbidity. To avoid damage of critical structures, such as major vessels or nerves, and to minimize donor site morbidity, knowledge of the anatomy of the lower limb, where the freestyle flap is to be elevated, is helpful. Ideally, a backup flap should also be available in the region where the incision is planned to facilitate conversion to the backup procedure when needed. In our experience, perforators larger than 0.5 mm can reliably be dissected and micro-anastomosed. Freestyle perforator flaps can be raised as local, regional, or free flaps.
Freestyle local flaps are considered more technically demanding and challenging than conventional flaps. The risk of flap failure decreases with a surgeon’s increasing experience and comfort in techniques required for perforator flap dissection under loupe magnification or the microscope. However, disadvantages include the possibility of inaccurately mapping the location of a skin vessel and the inability to predict the pedicle length. For these reasons, surgeons always need a backup plan.
Surgical procedures
Preoperative Skin Vessel Identification
Landmark for a freestyle local flap is the localization of the Dopplered skin vessels. We use the Super Dopplex II model number MD2/SD2 (Huntleigh Diagnosis, Cardiff, UK) connected to a VP10 (10 MHz). Perforator identification is essential to prevent random flap raising and is usually based on the presence of an audible Doppler signal. The more intense Doppler signal should be selected. The signal points should be preoperatively marked, ideally in the expected operative position to minimize discrepancies between audible signals and intraoperative findings. In distal limbs, signals from superficial perforators may overlap with signals from the axial vessel. In such cases, direct pressure on the skin surface with the Doppler probe or moving of the probe at the long axis with its head held at the same point, will alter the perforator signal and help to distinguish it from the axial vessel signal. Intraoperative exploration at the deep fascia plane through the wound edges of the defect or a noncommittal exploratory incision also can reveal suitable perforators supplying potential nearby local flaps, even without prior Doppler-aided mapping.
Flap Design
Flap design depends on the number and locations of detected skin vessels, defect size, regional anatomy, and donor site availability. The originally selected skin vessel can be replaced by a more suitable one found intraoperatively, and the planned skin flap should follow the axiality of its source vessel whenever possible. The flexibility for modification of the size and shape of the skin flap should be maintained and a backup flap with common border should be prepared to cope with unexpected intraoperative findings or injury to the vascular pedicle. The backup flap also can be a free microsurgical flap. The final skin incision should be decided only after taking all skin vessels into consideration and choosing the most reliable one that is long enough to reach the defect. The flap can be advanced or rotated toward the defect, depending on the positional relationship between the pedicle and the defect. Taking care not to strangulate the dissected vascular pedicle, the skin flap can be rotated 180° to reach the defect (so-called “propeller flap”).
Dissection
The dissection can be performed in a suprafascial or a subfascial plane. The perforator is then skeletonized under loupe magnification down to the source vessel. Preserving a tissue cuff surrounding the perforator prevents pedicle stretching during harvesting. If more than one skin vessel is found, the best one is selected with various criteria, such as pulsatility, size, number and size of accompanying veins, proximity to the defect, subcutaneous course, and difficulty of donor site closure. Applying microclamps on minor pedicles could assist this decision. Preservation of more than one perforator is advisable, but rarely feasible because of restricted flap movement.
All vessel branches should be meticulously cauterized or ligated with hemoclips to achieve the best possible hemostasis, which allows the surgeon to clearly visualize all skin vessels and important structures. During the dissection, the vascular pedicle should be irrigated with normal saline and lidocaine solution to maintain moisture and always be under minimal tension so that the arterial pulsation can be observed throughout its entire length. If a tourniquet is used, complete exsanguination before tourniquet inflation should be avoided to ensure that blood vessels remain full to assist the dissection. Once a sizable skin vessel is detected by Doppler ultrasonography and confirmed intraoperatively, the freestyle flap can be harvested safely without fear of anatomic inconsistencies.
Postoperative care and expected outcome
Depending on the regions where the freestyle flap is harvested and the size and volume of the flap, the donor site is chosen in an area that matches the recipient site and has a favorable donor site location. The donor site is closed primarily or with skin grafting. Future procedures such as serial excision or tissue expansion allow for excising the skin graft if needed.
Management of complications
Freestyle propeller flaps are popular in lower extremity reconstruction; however, their reliability remains uncertain and they have relatively important complication rates. The main complication is venous congestion, which frequently leads to venous necrosis and sometimes total flap failure. Salvage procedures include venous supercharging or conversion into a free flap transfer using the microsurgical technique.
Revision or subsequent procedures
The type of tissue transferred can be selected according to the requirements of the recipient site. Usually, freestyle flaps are harvested from the area around the defect, which has the same color, texture, pliability, and thickness. However, in case of bulky flaps, debulking procedures can be done at least 3 months after the flap reconstruction for optimal cosmetic results. These include staged excision, suction lipectomy, or 1-staged full-thickness skin grafting.
Case demonstrations
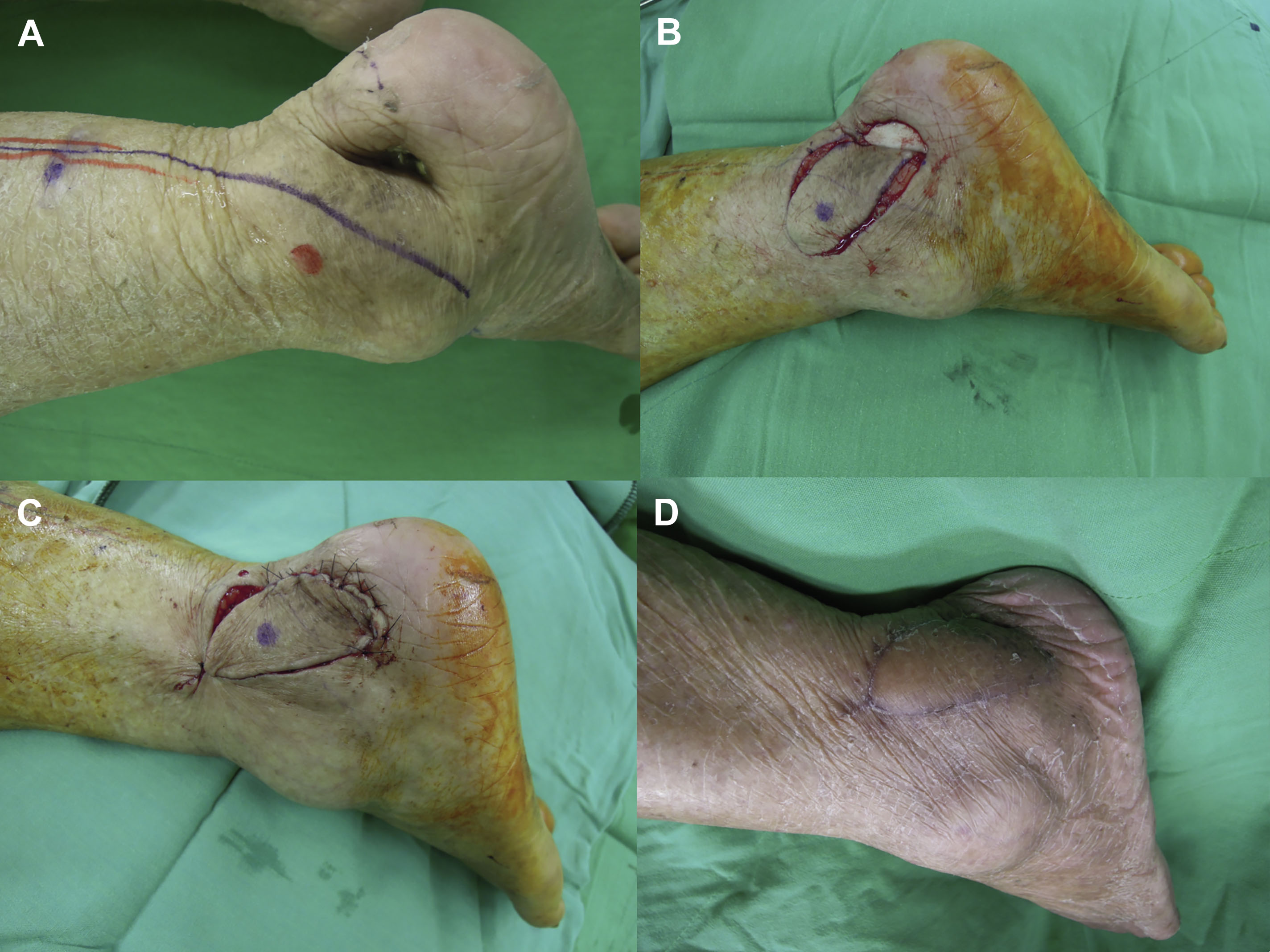
Case 1
Freestyle local V-Y advancement flap for coverage of a chronic ulcer of the lateral retromalleolar region with underlying osteomyelitis: (1) the marking line indicates the initial flap design; (2) by means of a handheld Doppler device, an audible perforator was marked; the advancement flap is elevated; (3) flap advancement into the defect and tension-free wound closure; (4) long-term result with uneventful wound healing 6 months after the operation ( Fig. 1 ).
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Free Flaps in Lower Extremity Reconstruction
Free Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


