Chronic lower extremity wounds are defined as wounds that fail to heal within 3 months of defect onset. Free tissue transfer offers an opportunity for limb salvage and length preservation. Preoperative optimization includes a medical and nutritional consult, complete work-up by vascular surgery, and an analysis of bony stability and gait biomechanics by podiatric surgery. In the authors’ practice, the thigh has proved the workhorse donor site and offers fasciocutaneous and muscle-based flaps depending on defect characteristics. Postoperative care requires early monitoring for flap compromise and continued long-term follow-up for wound recurrence.
Key points
- •
Patient optimization with multidisciplinary care, including vascular surgeons to address local ischemia and podiatric or orthopedic surgeons to address bony stability and biomechanics, is critical for long-term, durable flap success.
- •
Successful surgical management of chronic lower extremity wounds relies on aggressive surgical débridement to achieve a healthy wound bed.
- •
Wound closure with free tissue transfer preserves limb length, promotes ambulation, and reduces mortality in a highly comorbid population.
Introduction
Chronic wounds of the lower extremity can be defined as wounds that fail to regain normal functional and anatomic characteristics within 3 months. Recent data indicate that chronic wounds affect as many as 1% to 2% of the population in developed nations, with rates increasing as the population ages and becomes more comorbid. , Steady increase in this pathology makes the economic impact wide and far-reaching. Among Medicare beneficiaries, 15% of patients are diagnosed with chronic wounds, which is estimated to cost Medicare $28.1 billion to $96.8 billion per year for infection control, surgical procedures, and continued wound care.
The effect of lower extremity wounds is devastating to patient quality of life, pain measures, and, ultimately, survival. Patients with chronic wounds consistently score lower on patient-reported outcomes for physical functioning and pain. When wounds are persistent and progressive, risk for major lower extremity amputation (LEA) increases. For diabetics, chronic lower extremity wounds have a mortality rate of 43% to 55% within 5 years. After major LEA for any chronic wound, however, mortality rates increases to nearly 80% at 5 years, likely due to decline in functional ability, increased cardiovascular exertion, and exacerbation of existing comorbidities. Accordingly, diabetic foot ulcers have surpassed diabetic coma as the primary driver of mortality in this population. Although a young healthy adult may recover from an amputation, a comorbid patient with a lower baseline ability to perform activities of daily living may not. Preservation of limb length not only has functional benefits but also survival benefits.
Providers should strive for early, definitive wound management with a multidisciplinary approach to soft tissue coverage. Up to 80% of major LEAs can be avoided when local flaps or free tissue transfer (FTT) is used for chronic wound closure. , Efficacious treatment relies on thorough medical and wound histories, complete physical examination, patient optimization, and appropriate selection of treatment modality. Management must be tailored to the individual patient, underlying disease process, and wound characteristics. Often, this requires careful coordination of both medical and surgical therapies for permanent wound closure. This article aims to outline the authors’ tertiary wound care center’s multidisciplinary approach to management of chronic lower extremity wounds with a specific emphasis on the value and success rate of FTT.
Indications and contraindications
Traditional contraindications to microvascular surgery include the presence of hypercoagulable disease, peripheral vascular disease, and severe uncontrolled comorbidities. A large majority of the chronic wound population, however, are afflicted by these pathologies, and many chronic wound patients can have successful reconstruction and salvage. The authors’ group begins with a comprehensive approach to patient evaluation and treatment selection. Absolute contraindications include intolerance of prolonged anesthesia, infections recalcitrant to débridement, complete absence of local vascular flow from a major artery, noncompliance, and pyoderma gangrenosum.
Historically, the guiding principles for lower extremity wound coverage came from the traditional reconstructive ladder, which originally was described by Mathes and Nahai. Simple techniques often are sufficient for small or superficial ulcers on a non–weight-bearing surface. These include primary closure and closure with skin grafts. Attempting primary closure in areas of high tension with limited soft tissue mobility often is unsuccessful. Any wound with severe infection requires wide, radical débridement of biofilm. Wide regions of débridement and removal of nonviable bone and tendon obviates consideration of simple closure techniques.
Local flaps from intrinsic muscles of the foot offer limited tissue bulk for coverage and are limited to wounds that measure approximately 3 cm × 6 cm in size. The medial plantar flap is a common choice for local coverage of the foot. Unfortunately, significant mobility is difficult to achieve, limiting the utility of this flap, especially for posterior heel ulcers. Options for the distal third of the leg are especially limited in the vasculopath. The distally based superficial peroneal flap often has insufficient blood flow through the peroneal artery to vascularize the distal tip, which generally is the most needed area. Options for middle leg include the gastrocnemius, soleus, and tibialis anterior turnover flaps. In the proximal leg, the gastrocnemius has proved to be the workhorse flap. Fasciocutaneous flaps, however, may be ideal in highly active patients to limit donor site morbidity. Local coverage options are reserved for the unique case where the amount of devitalized tissue is limited.
Due to the limitations of primary closure, graft placement, and local flaps for chronic lower extremity wound treatment, a better modus operandi is the reconstructive elevator, first suggested by Dr Gottlieb in 1985. By proceeding to FTT, this approach to wound treatment restores durable form and function resistant to high levels of shear forces in the ambulatory patient. In the patient with a lower extremity wound, the lower rungs of the reconstructive ladder may succumb to friction with shoe wear or ambulation, resulting in surgical wound breakdown.
Perioperative evaluation and special considerations
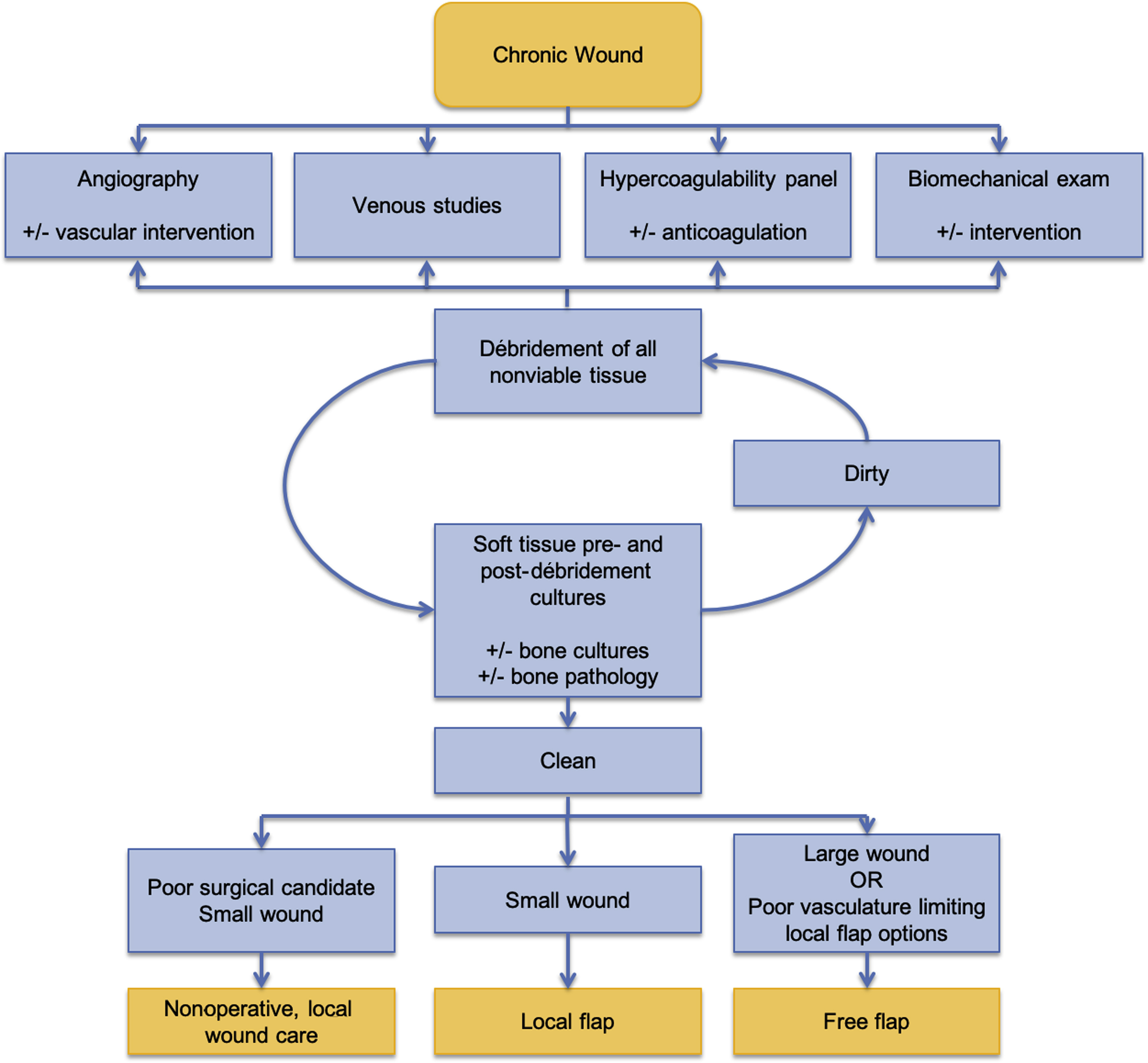
The authors’ management algorithm ( Fig. 1 ), requires multidisciplinary collaboration, radical surgical débridement to achieve a culture negative wound bed, angiography to define vasculature anatomy, vein studies to identify reflux, hypercoagulable studies to determine propensity for perioperative thrombosis, and a biomechanical examination to identify and address mechanical factors that propagate lower extremity wounds. Table 1 outlines characteristics of patients presenting to the authors’ wound clinic for limb salvage with FTT. Clinics serving a similar population may adapt the authors’ strategy to patient evaluation to suit their needs.
| Characteristic | Average (SD) or N (%) |
|---|---|
| Demographics | |
| Age | 55.5 (14.7) |
| Gender | |
| Female | 61 (29.0%) |
| Male | 149 (71.0%) |
| Body mass index | 29.21 (6.25) |
| Smoking | |
| Yes | 97 (46.2%) |
| No | 113 (53.8%) |
| Comorbid conditions | |
| Diabetes | 114 (54.3%) |
| Peripheral vascular disease | 48 (22.9%) |
| Congestive heart failure | 11 (5.2%) |
| Chronic obstructive pulmonary disease | 4 (1.9%) |
| Cerebrovascular accident/transient ischemic attack | 13 (6.2%) |
| Vascular Status | |
| Deep venous thrombosis | 6 (2.9%) |
| Venous reflux | 70 (33.3%) |
| Arterial vessel supply to the foot | |
| One vessel | 27 (12.9%) |
| Two vessels | 53 (25.2%) |
| Three vessels | 130 (61.9%) |
History and Physical Examination
Because comorbid conditions are known to inhibit wound healing and prevent FTT success, these pathologies must be identified through a thorough patient history and any preexisting conditions must be optimized before surgery. Table 2 outlines the main conditions posing concern.
| Medical history | Diabetes: hemoglobin A 1c <6.5%, perioperative blood glucose <200 mg/dL |
| Smoking: encourage to quit, must abstain for at least 6 wk | |
| Nutrition: prealbuminshould be tracked in the perioperative period | |
| Vascular examination | Ankle-brachial index |
| Angiogram | |
| Venous duplex ultrasound | |
| Biomechanical examination | Gait |
| Foot position | |
| Range of motion | |
| Infection control | Serial débridement |
| Culture-guided antibiotics | |
| Thrombophilia evaluation | History of thrombotic event |
| Preoperative thrombophilia panel | |
| Institute anticoagulation by risk stratification |
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Microsurgical Reconstruction of the Lower Extremity in the Elderly
Microsurgical Reconstruction of the Lower Extremity in the Elderly
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


