Improved knowledge of vascular anatomy has enabled surgeons to preoperatively identify perforators and design free-style flaps based on that perforator. Options for choosing the optimal donor site tissues are increased with the free-style technique. This reduces donor site morbidity while providing the same reconstructive success as traditional free skin flaps. The free-style technique allows the surgeon to successfully complete reconstruction when aberrant anatomy is encountered. With the necessary skills in perforator flap dissection and supermicrosurgery, the armamentarium of the reconstructive microsurgeon has been expanded with the introduction of free-style perforator free flaps.
Key points
- •
The Free-style free perforator flap can be a good option for lower extremity reconstruction.
- •
Free-style free flaps serve a valuable role when aberrant anatomy is encountered.
- •
Donor site morbidity is minimized with the versatile nature of free-style perforator flaps.
- •
Preoperative identification of perforators and their course may help to facilitate surgical dissection of the flap.
- •
The reconstructive surgeon should have knowledge of free-style flaps and be skilled at perforator dissection.
Introduction
Perforator flap surgery has greatly grown in popularity since first description by Koshima and Soeda in the 1980s. Their early innovation lead to the description of perforator flaps, advancing microsurgical reconstruction beyond fasciocutaneous and musculocutaneous free flaps. Perforator flap surgery reduces donor site morbidity by sparing underlying muscle and may allow for a more aesthetically pleasing reconstructive result. Much of the early innovation in traditional and free-style perforator flaps has been pioneered by colleagues in Asia. This was taken further when Wei and Mardini described the concept of a free-style free flap in 2004, in which a cutaneous perforator was identified with Doppler ultrasonography in the desired donor tissue and dissected retrograde to the source vessel. This surgical innovation has been made possible by advanced knowledge of perforator anatomy.
A landmark anatomic study by Taylor and Palmer in 1987 described over 350 major perforating vessels sized 0.5 mm or larger throughout the body, leading to the angiosome concept. The vascular territory of these perforators and their dynamic interplay with other nearby perforators via linking vessels are complex. Detailed anatomic studies have built on these findings, showing that each perforator has its own vascular territory, described as the perforasome theory. The perforasome theory proposes that a skilled surgeon can design a skin flap from almost any part of the body where a suitable perforator can be identified. , The primary limiting factors are the diameter and length of the source vessel. Free-style pedicled flaps can also be used for reconstructive surgery based on the same perforasome theory, and similarly are limited by location of the pivot point perforator relative to the defect. , However, the use of perforator flaps for free tissue transfer has overshadowed their utility as pedicled flaps. For example, traditional fasciocutaneous perforator flaps such as an anterolateral thigh perforator (ALT) flap have been shown to be useful in lower extremity reconstruction. This article highlights the utility of free-style free perforator flaps in lower extremity reconstruction. With adequate knowledge and surgical skill for free-style perforator flaps, the surgeon can also achieve an equally good outcome for lower extremity soft tissue coverage when those flaps are used as an alternative to a classic free perforator flap.
Indications and contraindications
Use of a free-style free perforator flap can be indicated for any lower extremity wound that requires reconstruction with a microvascular fasciocutaneous free flap. This technique is particularly useful when preoperative identification of vessels for traditional flaps such as the ALT perforator flap using handheld Doppler, duplex sonography, or other imaging modalities does not identify perforators of good caliber in the usual location. Because the thigh is a good donor site as a free skin or fasciocutaneous flap, a free-style free perforator flap can be designed in the same flap donor site of an ALT flap as long as a large and reliable perforator can be identified. Using principles of free-style perforator flaps, aberrant anatomy encountered during perforator flap dissection still allows for successful flap elevation after intramuscular pedicle dissection. Obviously, free-style free flaps should not be attempted if a suitable perforator cannot be identified or if the donor site does not have adequate tissue. Other contraindications for a free-style free perforator flap are the same as other free flap lower extremity reconstruction.
The timing for a free-style free perforator flap lower extremity reconstruction is the same as other free flap reconstruction in the lower extremity. Besides the patient’s readiness and associated medical conditions, a definitive soft tissue reconstruction is commonly performed within 7 to 10 days after initial consultation. With vacuum-assisted wound closure, the timing for free-style free perforator flap reconstruction can be prolonged to up to 3 weeks.
Preoperative evaluation and special considerations
Preoperative evaluation for a free-style free perforator flap is the same as for most lower extremity microvascular soft tissue reconstructions. The wound must be thoroughly debrided of all infected and necrotic tissue and ready for soft tissue coverage. Suitable recipient vessels outside the zone of injury should be identified with preoperative duplex sonography, computed tomography (CT) angiogram, or formal angiogram. The size of the defect and bulk required are measured. Flap donor site is selected based on minimizing donor site morbidity, tissue quality, and expected aesthetic outcome. For lower extremity reconstruction, the thigh is commonly used, as it typically provides the most reliable source of soft tissue with minimal donor site morbidity.
Traditionally, a handheld Doppler probe is used to identify perforators in the region of interest. However, it is the senior author’s preference is to use color duplex sonography preoperatively to measure a perforator’s vessel caliber and map its 3-dimensional course. , Once the perforator of adequate size and even the status of its blood flow can be identified and the 3-dimensional course of a perforator’s anatomy is known, such a perforator can be used to design a free-style free perforator flap. The septocutaneous or musculocutaneous course of that perforator is also identified preoperatively, which may help to save time or to limit extent of the flap dissection. This enables easier dissection and is particularly useful in the obese patient in whom the perforator may have a long subcutaneous course. Color duplex sonography is a cheap, effective method to reliably identify a perforator for a free skin perforator flap or free-style free perforator flap.
Pedicle length must be strongly considered when designing a free-style free flap. Ideally, the flap will be designed on a perforator that is far away from the source vessel. By doing so, the shortest pedicle will be the straight distance between the identified perforator and the source vessel. For example, in the thigh, this source vessel can be the superficial femoral artery or the profound artery.
Flap design is based on the location of the perforator(s) identified. Ideally, more than one perforator should be included in the flap design. The flap axis should be designed in the same orientation as that of the perforator linking vessels. This is axially in the extremities and along the axiality of muscles perpendicular to the midline on the posterior trunk and chest.
It is recommended that a conventional perforator flap such as an ALT flap be dissected first. Such a flap likely has more consistent perforators and is reliable for a safe flap dissection. If those typically more consistent perforators of the flap are found to be too small or insufficient blood flow, any larger sized perforator within the flap territory could be explored. It may serve as the perforator for a free-style free perforator flap even if it is not centrally located. A free-style free perforator flap should not be thought of as improvisation, but as an additional option in the microsurgeon’s armamentarium.
In the obese patient, it is the senior author’s preference to use a traditional free muscle flap with split-thickness skin graft in the management of complex lower extremity wounds. Although free muscle flaps atrophy and conform to the tissue, any perforator flaps in obese patients are difficult to perform and indeed require multiple debulking and revision procedures after initial flap reconstruction.
Surgical procedures
The free-style free perforator flap is the next level of flap choice for reconstruction of a lower extremity wound and may need additional surgical skill for the flap dissection. Certain reliable imaging studies for the perforator’s anatomy can be helpful, because the length of intramuscular dissection and the potential diameter of the pedicle can be estimated prior to the flap dissection. In that way, the surgeon can estimate whether the free-style free perforator flap can be harvested as a free skin flap for free tissue transfer. The common donor site is still in the thigh for most patients.
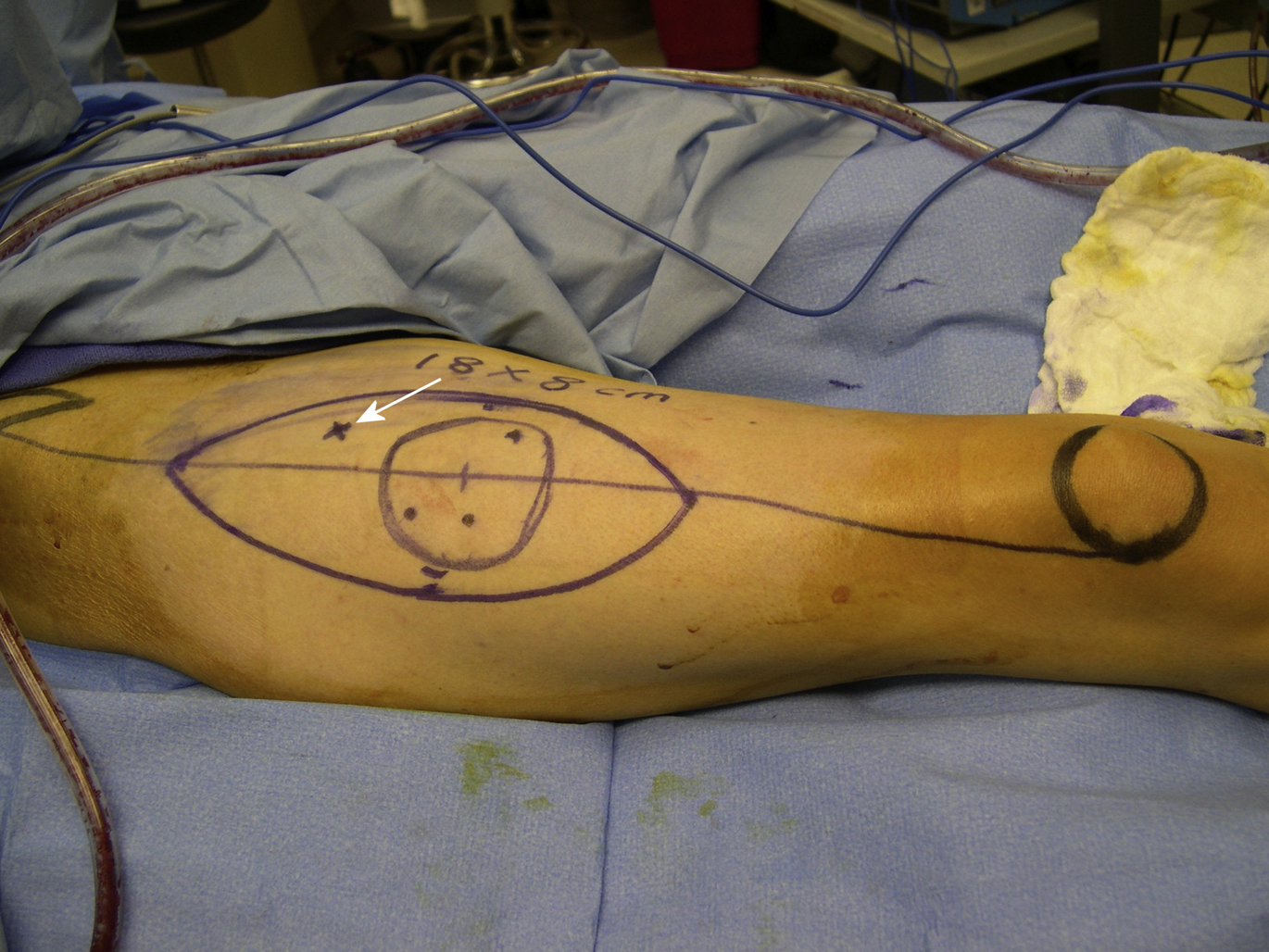
In the senior author’s practice, preoperative mapping of perforators with a color duplex scan is performed first, and at least 1 good perforator can be identified. Such a perforator may not even be centrally located if it is within the flap territory and has a good blood flow. The skin paddle of the free-style free perforator flap can be marked as the same as an ALT flap ( Fig. 1 ). The suprafascial dissection is performed first to explore the perforator ( Fig. 2 ). If the perforator appears to be larger (>1 mm in diameter) with good flow, sometimes with visible pulsation, further dissection around the perforator can be performed. During the perforator dissection, more attention should be paid for intramuscular dissection. Because it is unknown where the perforator would go inside a deep muscle, intramuscular dissection of the perforator can be tricky and difficult. The surgeon should be patient during the flap dissection and put proper traction on the perforator so that the intramuscular dissection of the perforator can be facilitated ( Fig. 3 ). Once the adequate pedicle length is achieved and the diameter of the pedicle is adequate for microvascular anastomosis, the pedicle can be divided, and a free-style free perforator flap dissection is completed ( Fig. 4 ). If the thigh is chosen as a donor site, the size of the skin island can be as large as 25 × 8 cm for subsequent primary closure ( Fig. 5 ). The average length of the pedicle is about 10 cm, but this can be tailored as long as the recipient vessel can be reached. However, the diameter of the pedicle can be quite small, and the surgeon who performs a free-style free perforator flap should feel comfortable performing microsurgery for the size of the vessel less than 1.5 mm in diameter ( Fig. 6 ). Often, an end-to-side arterial microvascular anastomosis is performed for such a small size of the pedicle artery from the flap. However, an end-to-end venous microvascular anastomosis can still be performed with a proper size of venous coupler ( Fig. 7 ).
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free Flaps in Lower Extremity Reconstruction
Free Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


