Free Lateral Arm Flap
John R. Lien
Kevin C. Chung
DEFINITION
The lateral arm flap is a reliable septofasciocutaneous flap for local and free tissue transfer.
Originally described for reconstructive head and neck coverage,1 the free lateral arm flap is useful for small to mediumsized defects of the hand and wrist.
ANATOMY
The arm is composed of anterior and posterior compartments.
Anterior compartment includes the biceps, brachialis, and coracobrachialis muscles.
Posterior compartment includes the triceps muscle.
The lateral intermuscular septum divides the anterior and posterior compartments laterally.
At the midpoint of the humeral shaft, the profunda brachii artery and radial nerve are located within the spiral groove of the humerus.
The profunda brachii divides into two main branches within the spiral groove: the radial collateral artery (RCA) and middle collateral artery (MCA).
The RCA accompanies the radial nerve and branches into the anterior and posterior radial collateral arteries (ARCA and PRCA) (FIG 1).
The PRCA is the nutrient artery for the lateral arm flap, feeding septocutaneous perforators along the lateral intermuscular septum.
The PRCA is accompanied by one or two venae comitantes.
The posterior antebrachial cutaneous nerve (PACN) branches from the radial nerve and accompanies the PRCA.
PATIENT HISTORY AND PHYSICAL FINDINGS
Assess for prior trauma or surgery at the potential donor site.
Ensure adequate recipient site debridement.
IMAGING
Doppler sonography can be used to ensure intact vascular pedicle and perforators in cases with prior trauma/surgery, but we generally avoid this flap in this situation.
SURGICAL MANAGEMENT
Lateral arm flap is indicated for coverage of small to mediumsized defects of the volar and dorsal wrist and hand.
Maximum skin island size is 8 × 25 cm, as the flap can be extended distal to the lateral epicondyle along the lateral forearm. Primary donor-site closure is dependent on body habitus, but generally 6 cm width can be closed primarily.
Obese patients will have a bulky lateral arm flap that may be cosmetically unappealing in the hand and wrist.
The PRCA pedicle is generally limited to 6 cm in length.
For extremity reconstruction with bone defect, a vascularized segment of distal humerus may be included in the flap.2
Doppler examination is used to center the skin paddle over the vascular pedicle.
The patient is placed supine with the hand on a hand table.
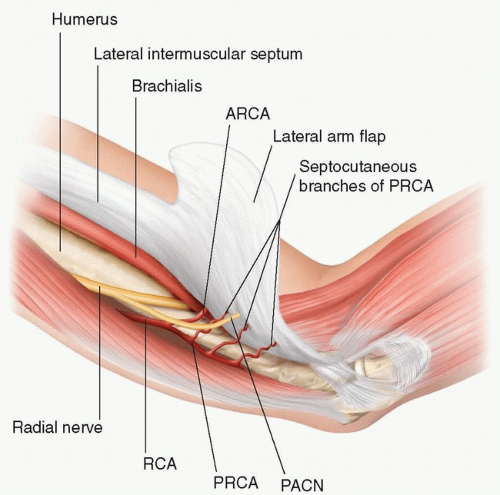 FIG 1 • Anatomy of the lateral arm flap. |
TECHNIQUES
▪ Flap Design
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


