Free tissue transfer to the lower extremity for limb salvage remains challenging. A comprehensive approach includes patient selection, flap selection, selection of the recipient vessels, flap dissection, flap preparation, microvascular anastomosis, flap inset, immediate postoperative care, intermediate postoperative care, and further follow-up care. Each step in this comprehensive approach has its unique considerations and should be executed equally to ensure an optimal outcome. Once acquired, some clinical experience along with adequate microsurgical skill, good surgical judgment, well instructed and step-by-step intraoperative execution, and a protocol-driven practice, successful free tissue transfer to the lower extremity can be accomplished.
Key points
- •
Free flap lower extremity reconstruction remains challenging to plastic surgeons.
- •
A comprehensive approach has been developed to ensure better clinical outcomes.
- •
Each step in the comprehensive approach has its unique considerations.
- •
A second free tissue transfer can also be performed successfully if the cause of the failure for the first free tissue transfer can be identified.
- •
There is a learning curve for free flap lower extremity reconstruction.
Introduction
Free tissue transfer to the lower extremity provides a critical means for limb salvage after orthopedic trauma or extensive tumor resection. With many recent advances in reconstructive microsurgery, a successful free tissue transfer can be achieved for soft tissue reconstruction of the lower extremity. , Frequently, free tissue transfer to the lower extremity may be the only option for limb salvage in patients with a complex traumatic wound.
The overall success rate of free tissue transfer to the lower extremity is still lower than to the head and neck or breast, even from some of the best microsurgery centers in the country. This may be due to several important factors. For example, massive edema of the leg is frequently present after trauma and abnormal or thrombogenic recipient vessels are a common problem secondary to peripheral vascular disease or traumatic injury. Therefore, the failure of free tissue transfer to the lower extremity remains relatively common and limb salvage for certain patients is still challenging to many plastic surgeons.
In this article, issues related to perioperative care of lower extremity free flap patients are discussed. The author’s comprehensive approach of free tissue transfer to lower extremity is also described in detail ( Box 1 ). With many recent advances in reconstructive microsurgery, it is possible that the clinical outcome of free tissue transfer to the lower extremity can be improved.
- 1.
Patient selection
- 2.
Flap selection
- 3.
Selection of recipient vessels
- 4.
Flap dissection
- 5.
Flap preparation
- 6.
Microvascular anastomosis
- 7.
Flap inset
- 8.
Immediate postoperative care
- 9.
Intermediate postoperative care
- 10.
Further follow-up care
Indications and contraindications
The classic indication for free flap lower extremity reconstructions in the author’s practice is an extensive wound in the distal third of the leg. In addition, a free flap is frequently indicated for an extensive wound in the upper or middle third of the leg or in the foot and ankle. A free flap is also indicated for a more complex wound in the lower extremity or a large wound with composite tissue loss. The timing of a free flap lower extremity reconstruction usually depends on the patient’s readiness and associated medical conditions. In general, a definitive soft tissue reconstruction is commonly performed within 7 to 10 days after initial consultation. However, with vacuum-assisted wound closure, the timing for such a reconstruction can be safely prolonged for to up to 3 weeks.
The contraindications for free flap lower extremity reconstruction in the author’s practice are the following: The patient’s general medical conditions cannot tolerate a lengthy procedure under general anesthesia; major vascular or nerve injury in the lower extremity; and a large composite tissue loss in the lower extremity beyond possibility of soft tissue or bony reconstruction. In addition, significant loss of a muscle compartment, associated with a vessel injury, deep vein thrombosis, or a hypercoagulative state are relatively contraindications for a free flap surgery in the lower extremity.
Preoperative evaluation and special considerations
When a patient is evaluated for free tissue transfer to the lower extremity, his or her medical condition should be evaluated carefully, especially if the patient has an associated injury from trauma. Just like any other surgeries, major surgical risks include previous heart attack, stroke, severe diabetes, uncontrolled hypertension, and significant hepatic or renal insufficiency. Many orthopedic trauma patients are commonly started on anticoagulation agents. Therefore, proper management of anticoagulation therapy for these patients perioperatively can be important to ensure a successful free tissue transfer. It may also be critical to screen certain patients for a hypercoagulable state if they have a history of recurrent vessel thrombosis or embolism or a recent splenectomy, because patients with a hypercoagulable state are very poor candidates for free tissue transfer. An appropriate hematologic consultation may be needed for those patients.
There are several issues that need to be considered for a free flap selection. In general, soft tissue requirement, availability of the flap tissue, and adequate length and size of the flap pedicle are the first 3 important considerations. It has been the author’s philosophy that a vein graft should be avoided if possible, for free tissue transfer to the lower extremity because of the added complexities and risks of venous anastomotic thrombosis. It is also important to select a flap that has minimal donor site morbidities. Sometimes, a surgeon’s familiarity with the flap may also be an important factor in flap selection. The commonly used flaps for lower extremity reconstructions in the author’s practice are the anterolateral thigh perforator (ALT) flap, or latissimus dorsi, rectus abdominus, and gracilis muscle flaps. The ALT flap has recently been used more frequently in soft tissue reconstruction of the lower extremity, representing a paradigm shift in the flap selection, because most microsurgeons including the author are now familiar with the ALT flap and the flap dissection becomes more successful, even it is still technically challenging. Other perforator flaps can also be selected based on the surgeon’s preference and familiarly with the flap.
Surgical procedures
Recipient Vessels Selection
When one considers the selection of recipient vessels, the surgeon should pay attention to both the artery and the vein because it is common that the flap loss is due to venous thrombosis. Therefore, an adequate size and quality of the vein without proximal obstruction is equally important as the artery to serve as a recipient vessel. Avoiding the “zone of the injury” is another important consideration for selection of recipient vessels in free flap lower extremity reconstruction. Lower extremity angiography or computed tomography angiography have been used routinely in the author’s practice as a baseline test to evaluate recipient vessels, especially for orthopedic trauma patients. If the surgeon has any suspicion about potential trauma to recipient vessels or deep venous thrombosis, the accompanied vein should also be evaluated separately by duplex scan or venography.
For lower extremity free tissue transfer, it has been the author’s preference that one should try to perform an end-to-end anastomosis if possible, even for the artery. This can be true if the anterior tibial artery or dorsalis pedis artery is chosen as a recipient vessel because an end-to-end arterial microanastomosis is considered technically easier by most surgeons, although there are no clear data to show that an end-to-end anastomosis would have better outcomes than end-to-side anastomosis.
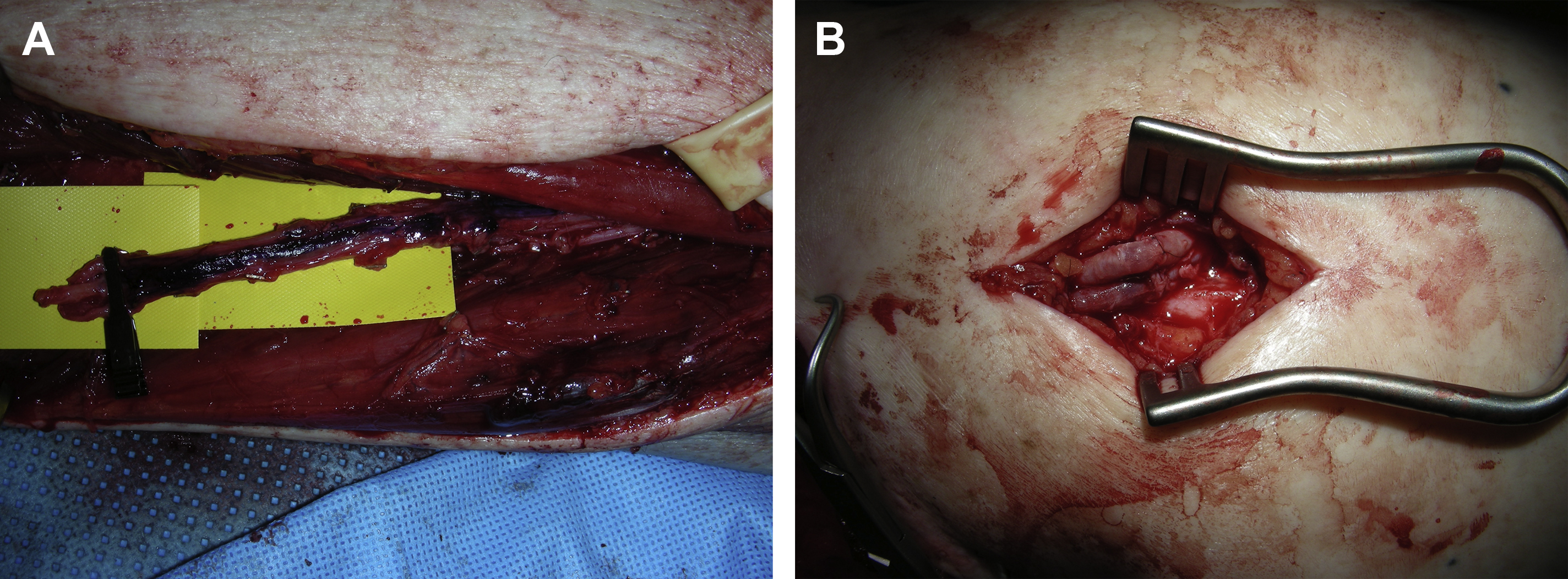
As indicated, the descending branch of the lateral circumflex femoral artery and vein or the anterior tibial artery and vein can be dissected free and used as recipient vessels in a turnover fashion for free tissue transfer to the difficult areas of the lower extremity, such as in the distal thigh or around knee ( Fig. 1 ). In that way, microvascular anastomoses for both artery and vein can be performed without difficulty and vein grafts can be avoided. ,
Flap Dissection
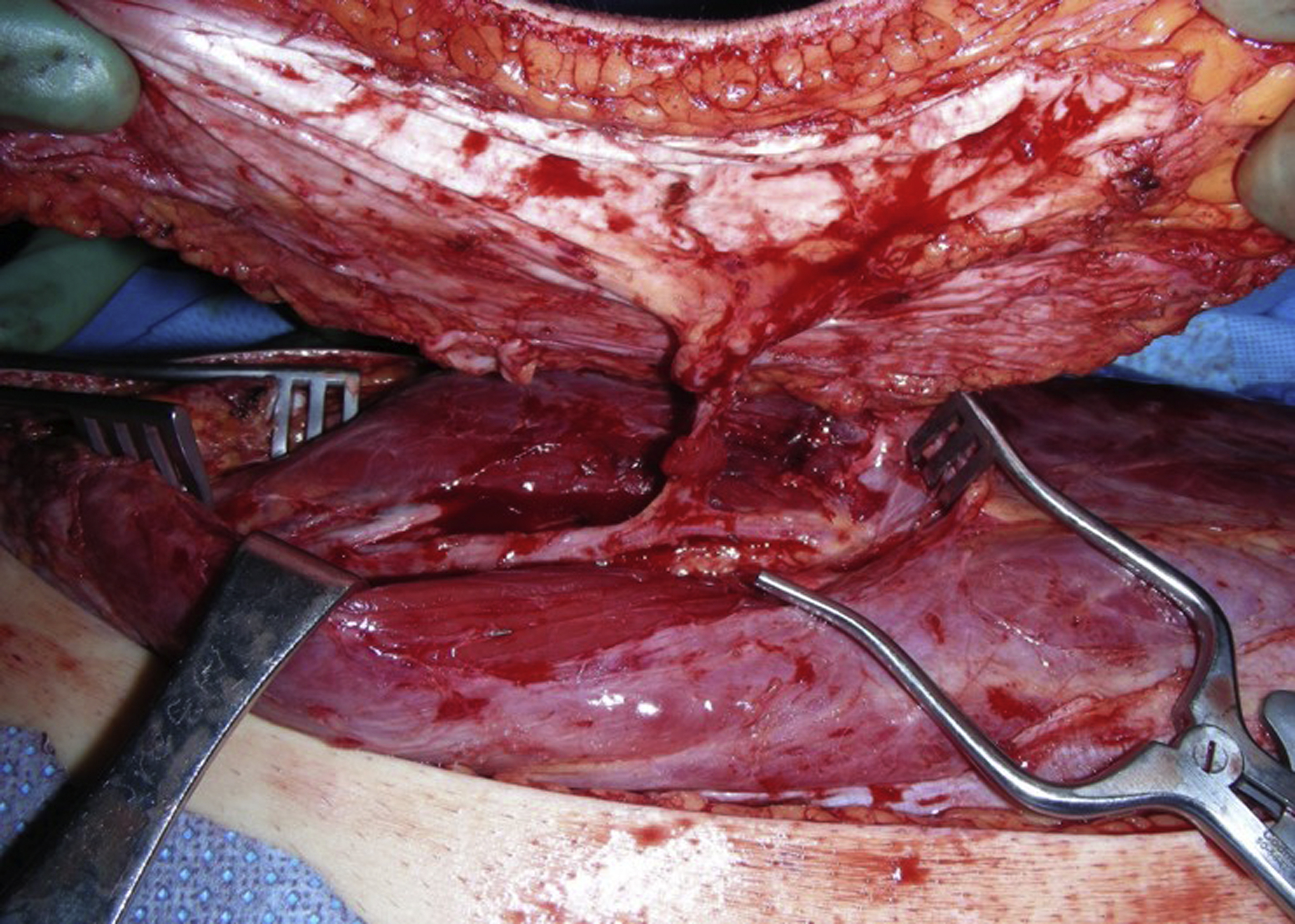
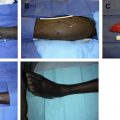
To ensure a relatively quick and easy flap dissection, the surgeon should know as much as possible about the detailed vascular anatomy of the flap before its dissection. This is particularly true for most perforator flaps. In the author’s practice, a duplex scan is routinely used for the preoperative mapping of the perforators, as well as the pedicle of the perforator flap before the flap dissection. In this way, the size and the number of the perforators that can be selected for the flap, the course of potential intramuscular dissection, and even the depth of the flap’s pedicle are evaluated. With this critical information in mind, a perforator flap, such as an ALT flap, can be elevated smoothly and safely. For an ALT flap dissection, the combination of retrograde and antegrade dissections of the pedicle can be performed for an easy flap dissection once the skin paddle of the flap is elevated ( Fig. 2 ).
Flap Preparation
The pedicle preparation of the flap can also be an important step in free tissue transfer. Once the pedicle of the flap is divided, it is the author’s preference that the artery of the pedicle is flushed with a higher concentration of heparinized saline (100 U/mL). In this way, the microvascular system of the flap may be loaded with heparin so that future thrombosis within the flap may be prevented without the systemic administration of heparin. The pedicle vessels of the flap is prepared under loop magnification. It is the author’s preference that the surgical preparation of the pedicle vessels be done mostly with surgical loops so that a lengthy preparation of the pedicle vessels under an operating microscope can be avoided.
In general, no systemic heparinization is needed for a routine free tissue transfer to the lower extremity in the author’s practice, although systemic heparin is still used by some surgeons before clamping vessels. Occasionally for the patient with severe peripheral vascular disease, heparinized saline may be perfused distally before the clamping of the recipient artery.
Microvascular Anastomosis
Microvascular anastomosis is a critical step for the success of free tissue transfer. After intense flap dissection and preparation of the recipient vessels, the surgeon should consider taking a break before the next intense part of the procedure (the microvascular anastomosis). It is the author’s belief that taking a short break (about 10–15 minutes) greatly enhances the microsurgeon’s performance for microvascular anastomosis under a microscope. There are also additional advantages for the patient while the surgeon takes a break. For example, the flap is allowed to rest and perfuse normally after flap dissection to restore normal perfusion, and the recipient vessels can be rested and recovered from vasospasm. In addition, hypothermia or hypovolemia, a common condition when a patient has been under general anesthesia for a longer period of time, can be corrected by the anesthesiologist while the surgeon is taking a break. Because of this break, the surgeon, the patient, the flap, and the recipient vessels are all in optimal conditions and, thus, the success of microvascular anastomosis can almost be guaranteed.
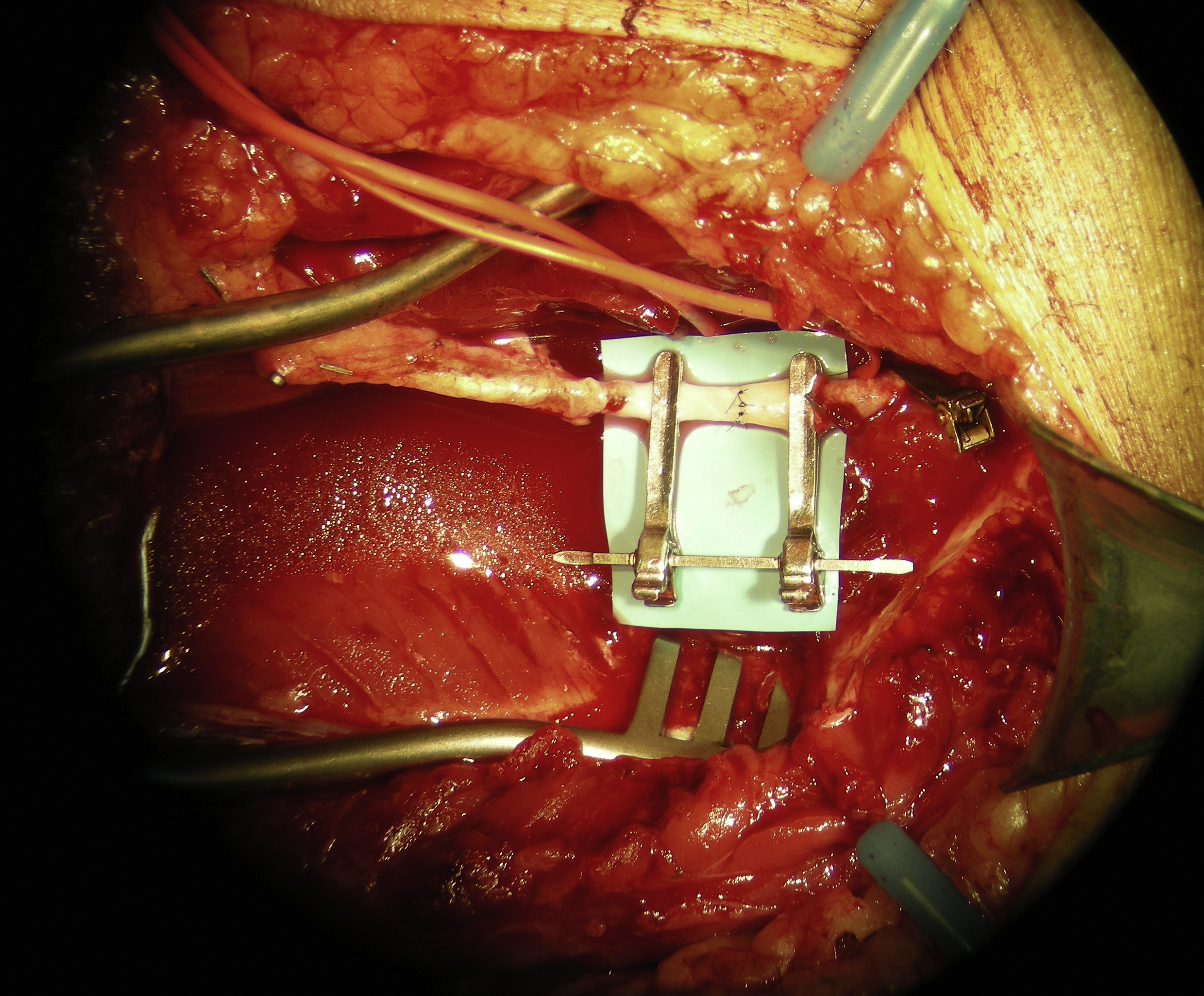
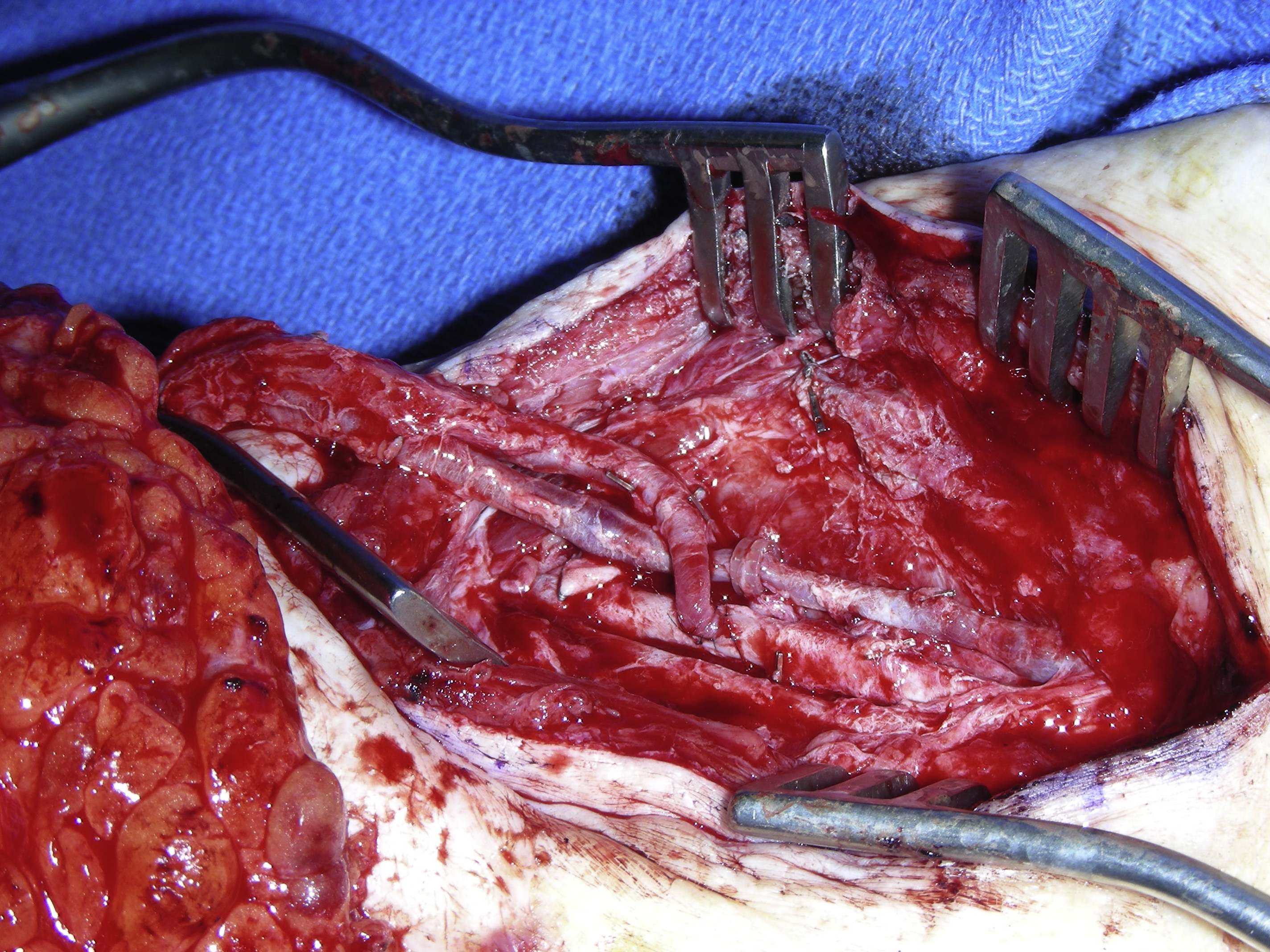
Before microvascular anastomosis, the surgeon should take time to set up the vessels. It is the author’s preference that a double-armed microvascular clamp is used to aid an end-to-end arterial microanastomosis ( Fig. 3 ). For an end-to-side arterial microanastomosis, an adequate size and shape of an arteriotomy over the recipient artery should be performed to ensure a successful end-to-side arterial microanastomosis ( Fig. 4 ). The author prefers to use an 8-0 nylon suture for routine arterial microanastomosis when the size of the pedicle artery is greater than 1.5 mm, resulting in fewer sutures needing to be placed to the anastomosis.
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


