Enhanced recovery after surgery (ERAS) protocols facilitates a standardized patient care regimen with a goal of reducing the metabolic stress of surgery. Adapted to head and neck free flap reconstructive surgery in 2017, these protocols focused on several key domains such as perioperative nutritional optimization, multimodal pain control, and early mobilization. Studies have shown that in addition to ERAS implementation, the maintenance and improvement of ERAS protocol compliance rates improve perioperative outcomes such as hospital length of stay and decrease major postoperative complications.
Key points
- •
Enhanced recovery after surgery (ERAS) protocols adapted to head and neck free flap reconstructive surgeries have proven to reduce duration of hospitalization and improve patient outcomes.
- •
The use of multimodal, perioperative, non-opioid analgesic medications has reduced post-operative pain scores and opioid use.
- •
Shorter (<12 hours) pre-operative fasting times and pre-operative carbohydrate loading combined with pre-admission malnutrition screening and nutritional pre-habilitation can lead to shorter hospital stays.
- •
Technological advances in computer assisted surgery have reduced operative times leading to reduced risk of post-operative complications.
- •
Preset perioperative order sets can help implement and increase compliance rates for ERAS protocols.
Introduction
Enhanced recovery after surgery (ERAS) protocols are a set of standardized multimodal perioperative recommendations first initiated in general surgery to improve patient outcomes and decrease complications. Recognizing the unique challenges faced by head and neck free flap surgery, ERAS protocols were adapted for head and neck oncologic surgery over the last decade. The implementation of ERAS protocols, in multiple international large-scale studies, has created a track record of improving key patient outcomes including length of stay (LOS) in the hospital, complication rates, and reduced opioid use. , This review summarizes the current evidence on ERAS interventions in patients undergoing head and neck free flap surgery.
Enhanced recovery after surgery implementation
ERAS protocol implementation is a time, energy, and cost-intensive process requiring the buy-in of multiple stakeholders. The team includes hospital administrators, surgeons, trainees, anesthesiologists, speech-language pathologists, social workers, dietitians, operating room surgical technologists, and nurses. The ERAS protocols compliance rate can be as low as 60% when implementation is poorly planned. When post-implementation interventions were enacted, the compliance rate rose to 89% and was shown to be inversely correlated with LOS.
Strategies , exist to successfully implement change in health care systems, including.
- 1.
Identifying navigators to coordinate the gathering of key stakeholders
- 2.
Identifying novel practices to be implemented
- 3.
Developing milestones of implementation to monitor progress of the change
- 4.
Integrating ERAS protocols into electronic medical records (EMRs)
Structured and planned educational sessions on the goals of ERAS can improve compliance, even with staff who have previously been exposed to ERAS protocols. , A successful ERAS program can effectively be considered as a long-term recurring quality improvement (QI) initiative, with the team regularly revisiting the results of implementation, monitoring/recording compliance rates, and revising protocols to address barriers/gaps that are identified. , The iterative cycle of improvement, highlighted in methods such as plan-do-study-act (PDSA) or Lean Six Sigma principles, may be particularly advantageous for the success of these types of initiatives and have a track record of being implemented in surgical QI projects and ERAS protocols. , The cycle of reinvestigation and improvement of ERAS compliance rates may take months to years but can offer benefits in long-term patient outcomes.
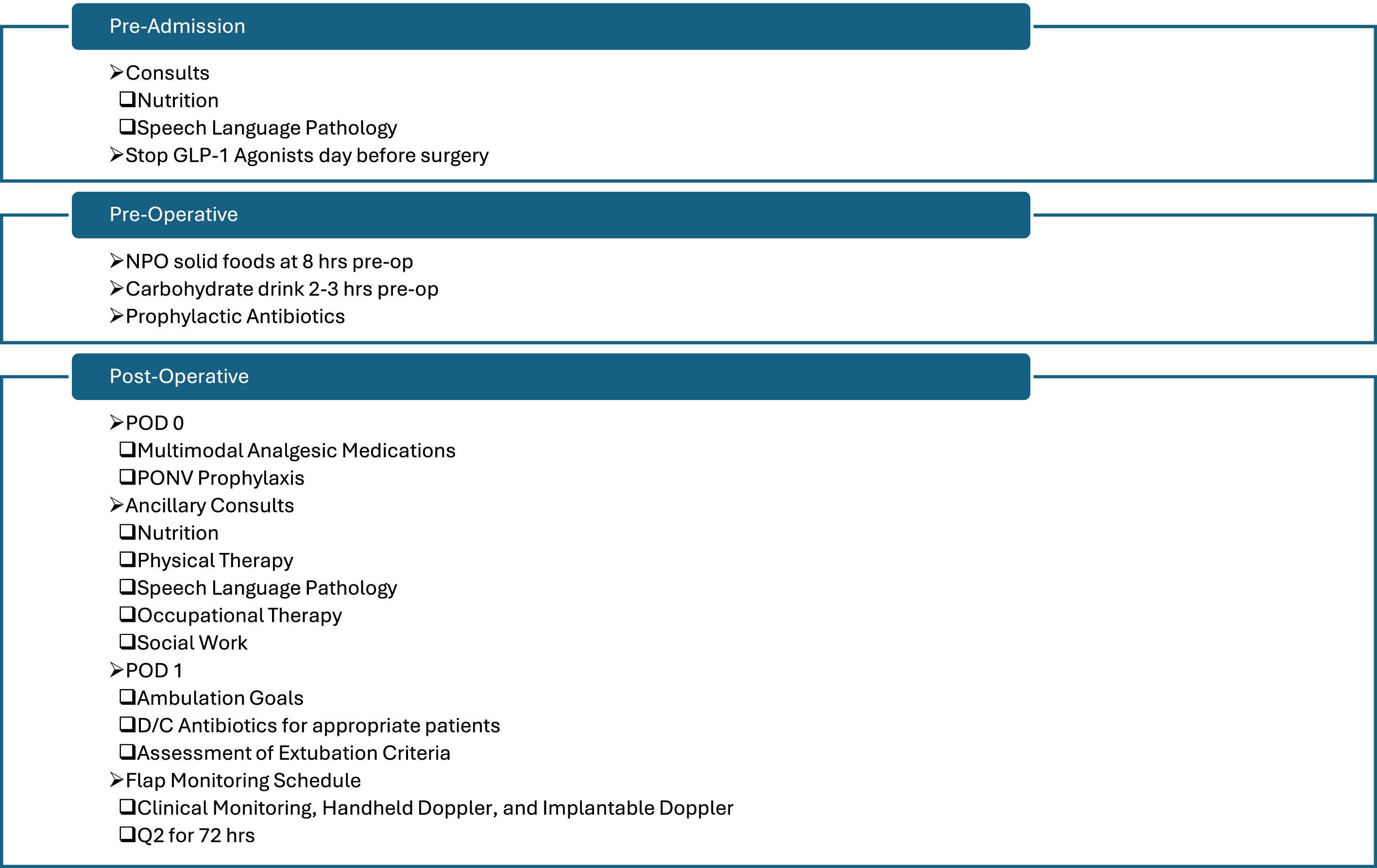
EMRs systems can be leveraged to increase compliance. Preset pre- and post-operative order sets in EMRs may force compliance and facilitate a shift in perioperative culture. Standardized order sets have been shown to reduce errors in complex order sets and improve compliance in key areas such as analgesia protocols and early mobility ( Fig. 1 ).
Pre-operative interventions
Patient Education
Patients undergoing head and neck free flap surgery are often faced with overwhelming amounts of information. Preadmission education can be a key intervention to prepare patients for their participation in pre- and post-operative protocols. These pre-operative encounters serve as ideal opportunities to educate patients on pre-operative goals and post-operative lifestyle changes. Both written information and visual illustrations can be utilized for increased understanding and recall. The augmented patient education sessions have been a mainstay of ERAS pre-operative education protocol and have been further supported by single-institutional trials and systematic reviews. , , ,
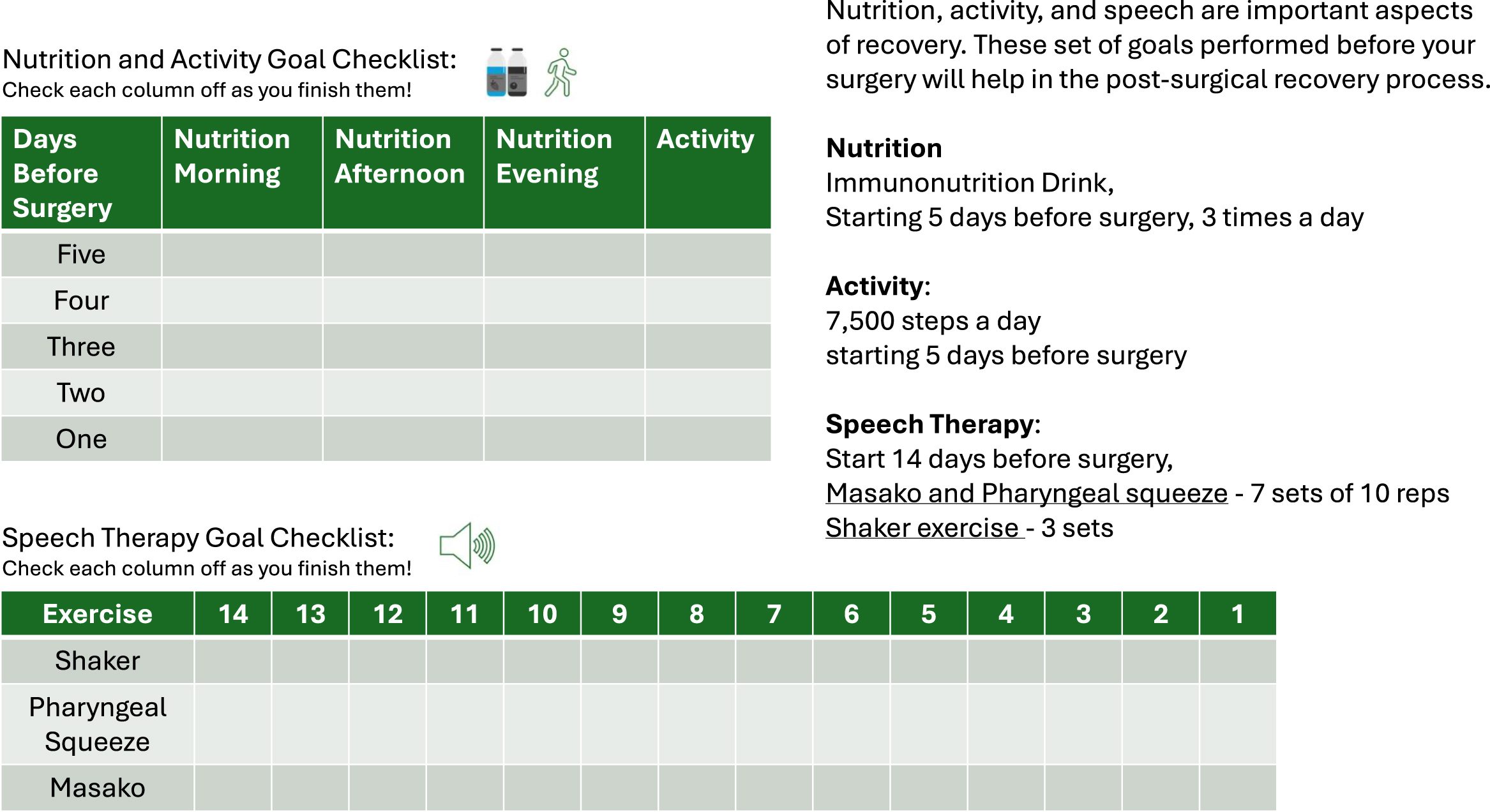
Recent evidence has begun to demonstrate the utility of defined “prehabilitation” programs, to help optimize a patient’s medical status prior to surgery. Adapted from information in Moore and colleagues 2021 and Virani and colleagues 2015, Fig. 2 is an example of a written prehabilitation protocol for patients undergoing head and neck free flap surgery. , In the supplemental materials, a pre-operative patient checklist ( [CR] ) and prescriptions checklist ( [CR] ) used at the author’s institution are available for reference and adaptation. In adapting a pre-habilitation protocol or creating new patient educational tools, a multidisciplinary approach with nutrition, speech-language pathology, and physical and occupational therapy is recommended to ensure the material accounts for the varied post-operative changes anticipated. Further care should also be taken to ensure readability for patient comprehension. , Future directions in patient education include creating audio-visual material, which has been shown to increase post-operative satisfaction with surgery.
Pre-admission Depression Screening and Tobacco and Alcohol Cessation
Incidence of depression in head and neck cancers ranges from 6% to 52% and is often under-diagnosed and under-treated. Furthermore, head and neck cancer patients have a nearly 2 fold higher risk of dying from suicide. , Depression can have a direct effect on compliance with treatment and overall survival. , Depression screening and referral to mental health consultation are critical to diagnosis, appropriate treatment, and reduction of symptomology. A population-based cohort study of over 55,000 patients diagnosed with head and neck cancer showed outpatient psychiatric care post cancer diagnosis improved overall survival (HR 0.80, 0.83–0.94 95% CI) when compared to patients not diagnosed with depression. For patients with depression before cancer diagnosis, sustained outpatient psychiatric care resulted in an improved overall survival rate compared to those with treatment interruptions; furthermore, those with an increased frequency of outpatient psychiatric care after cancer diagnosis also had an overall survival benefit. Prophylactic escitalopram prescribed to patients with a Quick Inventory of Depressive Symptomatology—Self Report score of 2 or greater may lead to a decrease in the development of depression. ,
The harms of tobacco and alcohol use, as well as the benefits of cessation, are well-documented. In the context of head and neck surgery, smoking cessation at least 4 weeks before surgery reduces the incidence of surgical site infections (SSIs); though this ought to be balanced with time to treatment to prevent the progression of cancer. At diagnosis, a combination of sustained counseling over time and cessation medication such as varenicline, bupropion, and nicotine replacement therapy (NRT) have shown to have long-term success in maintaining abstinence. Counseling and medical treatment for alcohol cessation should be performed concomitantly. Alcohol cessation protocols in head and neck cancer patients have been implemented and are successful at reducing complications and normalizing LOS. These can be integrated into the ERAS protocols. Large-scale studies outside of head and neck surgery have shown that NRT does not have any adverse effects. ,
Pre-operative Nutrition
Malnutrition, a broad term describing an imbalance in nutrition, including undernutrition, is commonly associated with head and neck cancer, especially in the elderly. Preoperative malnutrition can lead to immunosuppression, impaired wound healing, increased infection rates, high treatment costs, and overall increases in mortality, morbidity, LOS, and readmission rates. In the hospital setting, it is estimated that 20% to 50% of patients are malnourished, stemming from the patient’s reduced appetite, symptoms related to cancer, high metabolic demand from surgery, and antineoplastic treatment. ,
Head and neck cancer patients should be assessed for malnutrition using current gold standard criteria from the Global Leadership Initiative on Malnutrition (GLIM). , , The GLIM criteria are separated into phenotypic and etiologic criteria. Within phenotypic criteria, the patient is evaluated for weight loss, low body mass index, and reduced muscle mass. , The etiologic criteria assess for reduced food intake and the presence of disease-related inflammation. , A diagnosis of malnutrition is established when at least 1 of each criteria is met. , A malnutrition diagnosis is not only important for prognostication, but may also act as a modifiable risk factor, that if optimized, can help improve perioperative outcomes. Consultation with a dietitian is recommended in these cases to facilitate a comprehensive nutritional assessment and, potentially, the development of a personalized nutritional prehabilitation protocol. , , An aspect of nutritional habilitation is the use of specific nutrients to modulate the immune system, known as immunonutrition. Preoperative immunonutrition, often enriched with arginine, glutamine, ω-3 fatty acids, or ribonucleic acids, used in the setting of malnutrition can reduce post-operative complications and SSIs.
Pre-admission Speech Language Pathologist Assessment
Patients who undergo head and neck free flap reconstruction involving the upper aerodigestive tract often have both pre-operative swallowing dysfunction, related to the tumor, and post-operative functional changes, related to surgery. Pre-operative Speech Language Pathologist (SLP) evaluation can improve patient expectations and compliance with post-operative rehabilitation, and thus, improve nutrition and recovery. In addition, pre-habilitation with prophylactic swallowing exercises (PSEs) has shown to decrease time to oral intake and to reduce LOS in surgical oncology literature. Within head and neck cancers, prospective trials have demonstrated that PSEs in patients undergoing concurrent chemoradiation therapy (CRT) can improve swallowing function, increase oral intake, and decrease the rate of percutaneous endoscopic gastrostomy tube placement. , In patients undergoing transoral robotic surgery for oropharyngeal cancers, standardized SLP evaluation pathways have been shown to improve swallowing outcomes and significantly decrease the need for feeding tube use. This includes standardized pre-operative evaluation pathways for swallowing assessment. SLPs implemented PSEs as repetitive daily exercise regimens such as 7 sets of 10 repetitions of the Masako and Pharyngeal squeeze exercises with 3 sets of the Shaker exercise starting 2 weeks before initiation of CRT (see Fig. 2 ). Patients educated about their PSE regimen at an in-person session with a written and video instructions had compliance rates of 70% at 3 weeks. Though there were differences in timelines and exercises of PSE regimens, PSE implementation can be a cost-effective method to improve the quality of life for patients with head and neck cancer. Adherence to SLP exercises has also been shown to be better when supplemented with on-line virtual coaching.
Pre-Operative Fasting
Nothing by mouth (NPO) after midnight was initiated to minimize the risk of pulmonary aspiration in patients awaiting procedures requiring anesthesia and to prevent procedural delays by ensuring patient readiness. However, prolonged preoperative fasting increases the risk of dehydration, patient irritability, electrolyte imbalance, hypotension at the start of anesthesia, catabolism, insulin resistance, and hyperglycemia; in turn, this may increase the risk of SSIs, mortality, and LOS. Gastric studies have shown that most clear liquids will be out of the stomach within 2 hours, and the risk of aspiration with reduced pre-operative fasting time is quite low. , , The eradication of prolonged fasting can minimize the negative effects of pre-operative fasting on post-operative nutritional status.
The American Society of Anesthesiologists (ASA) supports the 2017 guideline recommendations: clear liquids up to 2 hours, nonhuman milk up to 6 hours, a light meal (ie, toast and clear liquids) up to 6 hours, and a fatty meal up to 8 hours pre-operatively. , Recent head and neck surgery ERAS studies implemented an exception in overnight NPO for high carbohydrate beverages 2 to 3 hours pre-operatively. , Several clear liquid options for carbohydrate-rich drinks are available and can be administered without an increase in post-operative complications secondary to aspiration such as pneumonia. , , Carbohydrate loading is thought to reduce insulin resistance resulting in better glucose control, lean tissue preservation, and reduced protein loss. , , A retrospective case-matched cohort study (n = 122) on patients undergoing head and neck tumor resection with reconstruction showed that pre-operative carbohydrate loading (8–10 oz of clear carbohydrate beverages) 2 to 3 hours before anesthesia was independently associated with shorter hospital stays by 1.39 days without an increase in surgical site infection or 30-day readmission rates. , Furthermore, oral nutritional supplementation has been associated with a low risk of aspiration due to maintaining low gastric volume on administration. Pre-operative carbohydrate loading was developed and safely utilized in other surgical specialties for decades, and recent studies in head and neck cancer patients have correlated these benefits. , , ,
Patients with decreased gastric emptying, gastric or bowel obstruction, or lower esophageal sphincter incompetence may have an increased risk for regurgitation or aspiration, and may require a longer than ASA guideline NPO time. Delayed gastric emptying can occur secondary to the use of glucagon-like peptide-1 (GLP-1) receptor agonists; thus, the ASA recommends holding GLP-1 agonists the day before surgery if the patient is on daily dosing, and 1 week before if on weekly dosing. Pending novel evidence on optimal fasting duration for patients taking GLP-1 agonists, the current fasting guidelines, including the use of carbohydrate loading 2 to 3 hours pre-operatively, should be followed.
Day of Surgery Medications and Preemptive Analgesia
Head and neck free flap patients benefit from multimodal analgesia on multiple fronts. Preemptive analgesia with nonopioid multimodal medications is an integral component of ERAS in head and neck surgery and other specialties. , A combination of celecoxib, tramadol extended release, acetaminophen, and gabapentin in head and neck cancer patients has demonstrated a decrease in post-operative pain scores, use of patient-controlled analgesia, and opioid dosage at discharge. , , , , Non-steroidal anti-inflammatory medications (NSAIDs) use, including celecoxib, has not demonstrated an increased risk of bleeding or hematoma formation in patients undergoing head and neck surgery with free flap reconstruction; however, recognition of contraindications such as pre-operative chronic kidney disease or post-operative acute kidney injury precluding their use is recommended. , ,
Gabapentin should be administered with caution to patients older than 65 years of age due to an increased risk of post-operative delirium and sedation. , These psychological side effects may be dose-dependent, and encouragingly, gabapentin dosing schedules of 300 mg every 8 hours, 600 mg on day of surgery, and 300 mg BID have been used in elderly patients in large-scale head and neck ERAS protocol studies without increased overall complication rates or reports of increased delirium or hallucination rates. , , ,
Most patients face moderate anxiety during the day of surgery that does not require treatment. However, managing the high anxiety nature of pre-surgical environments can increase patient comfort and reduce post-surgical pain scores. , For those who express high levels of anxiety, pre-operative pharmaceutical treatment via benzodiazepines such as midazolam is commonly used, though its effectiveness in anxiolysis remains debated. , Furthermore, the routine use of benzodiazepines is no longer recommended by the European Society of Anesthesiology. Non-pharmaceutical interventions such as a preoperative anesthesiology visit with education tailored to patient needs, music interventions provided during induction of general anesthesia, and preoperative oral carbohydrate solution have been shown to be effective in reducing anxiety and may be used in lieu of or in combination with pre-operative pharmaceutical measures. ,
Antibiotic Prophylaxis
Head and neck surgical sites are often clean-contaminated due to exposure to saliva, pharyngeal, and tracheal secretions. SSIs remain a common complication with an incidence rate from 3% to 41%. SSIs can lead to prolonged hospitalization and wound dehiscence or fistulae. The need for antibiotic prophylaxis is well established though the ideal combination and duration of antibiotic use remains in discussion. Ampicillin-sulbactam, cefazolin/metronidazole, and cephalosporins alone, such as cefazolin, cefoperazone, and cefotaxime, were found to be effective antibiotic prophylaxis in post-head and neck free flap reconstructive surgery. However, ampicillin-sulbactam is generally considered the prophylactic antibiotic of choice for clean-contaminated head and neck free flap surgery. Clindamycin and benzylpenicillin were not found to be effective and are not recommended for use in head and neck patients post-free flap surgery. Longer courses of antibiotics (>24 hours) have shown no increased benefit. , In surgical sites involving the mucosa, topical antimicrobial formulations such as chlorhexidine gluconate and povidone-iodine applied via oral rinses have been shown to reduce the SSI rate when compared to parenteral prophylaxis alone while decreasing oral bacterial colony forming units compared to pre-operative levels. The Center for Disease Control 2017 guidelines for the prevention of SSIs advise the use of alcohol-based antiseptics for pre-operative skin preparation. Chlorhexidine has demonstrated ototoxicity when contacting the inner ear and ought to be avoided in such situations. ,
The logistical burden of intraoperative redosing may be considered when choosing a parenteral antibiotic regimen to implement. Cefazolin/metronidazole has shown the highest rate of adherence in redosing in a single-center academic study. With a lack of general consensus in the literature specific to the head and neck free flap patient population and recognizing institutional variations, the authors recommend consulting with institutional infectious disease experts to choose the optimal local regimen.
Computer Assisted Surgery
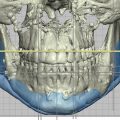
Computer-assisted surgery (CAS), specifically virtual surgical planning (VSP) with 3D surgical modeling, patient-specific templates, cutting guides, and implants, is transforming head and neck surgery in real time. , VSP use in certain head and neck free flap reconstructive surgeries, often involving osseous deformations, has led to a decrease in LOS, mean procedure and ischemia time, and an increase ease of operation and accuracy. VSP is one of the few interventions discussed that can potentially reduce operative time and thus, time under anesthesia, an independent risk factor for overall complications, surgical complications, and postoperative transfusions. , Furthermore, VSP has enabled novel, multidisciplinary, surgical procedures such as “jaw-in-a-day” that significantly reduces the morbidity faced by patients. In part due to operative time reduction granted by VSP use, surgeons can perform a dental and maxillofacial reconstruction in 1 day rather than months apart, saving the patient the morbidity of 2 separate operations and living without teeth in between cases. , Implementation of CAS in the context of the ERAS protocol has resulted in reduced operative time and average LOS. Despite the success of VSP in free flap surgery, factors such as high upfront cost with variable total cost estimates, administrative delay to generate pre-bent plates, and limited flexibility on the day of surgery remain barriers for incorporation and implementation into existing workflows. , , If barriers to implementation such as price or infrastructure need ease, CAS and VSP systems may become an essential part of ERAS. ,
Intra-operative interventions
The consistent implementation of ERAS protocols can be difficult in a multidisciplinary operative environment encountered during free flap reconstructive surgery. ERAS specific templates can be used to increase compliance. A safety checklist can be used at the beginning of the case during time-out to ensure all members are following the same standard. Anesthesia reference cards can help adherence to the protocol during shift change. Examples of both are included in the supplemental material ( [CR] and [CR] ), designed to be adapted in consultation with all stakeholders at your institutions.
Normothermia
Intraoperative hypothermia, defined as a core body temperature less than 36ºC, increases the risk of complications including SSIs, coagulopathies, blood loss, flap failure, arterial thrombosis, and prolonged LOS. Ideally, continuous core temperature should be monitored throughout surgery. Active warming is essential in free flap patients given the amount of skin exposure from multiple operative sites. Forced air warming devices can be started pre-operatively in addition to resistive heating blanket/mattress, and warmed intravenous and irrigation fluid utilized intraoperatively. , It is important to pay attention to limiting skin exposure when preparing the patient prior to final draping, since a drop in core body temperature can be common at this stage.
Intra-operative Fluid Management and Blood Pressure
Fluid status maintenance is key in minimizing post-operative complications. Common methods include the use of crystalloids, colloids, and vasopressors. As fluid overload increases the risk of flap failure, vasopressors such as ephedrine, phenylephrine, and norepinephrine can be used safely to maintain mean arterial pressure and improve tissue perfusion in head and neck surgery without risk of free flap failure. ,
Goal direct fluid therapy (GDFT) involves fluid resuscitation based on hemodynamic factors of stroke volume (SV) and stroke volume variation (SVV) to optimize cardiac output. , SVV, SV, Pleth variability index, and Central venous oxygen saturation (ScvO 2 ), among other parameters, can be used to monitor GDFT. Arterial pulse analysis, plethysmograph waveform analysis, thermodilution, and esophageal doppler and echocardiograms are the techniques used to monitor GFDT. Observational case-control studies have shown that GDFT monitored via SVV decreased the length of hospitalization and improved flap survival in head and neck surgeries. , However, consensus about its exact benefits, optimal hemodynamic factor to monitor, and optimal methods of monitoring have yet to be determined. , A commonly utilized method of monitoring in head and neck surgery is balancing fluid in versus urine out and blood loss.
Increased volume of infusion is associated with post-operative complications in head and neck surgery. , Patients who received greater than 5.5 L had a 2.9-fold increased risk for all post-operative complications, and those with greater than 7L were at increased risk for major complications such as flap failure or death. Additionally, a study by Farewell and colleagues showed patients with postoperative complications had an infusion of greater than 6L versus less than 3L for those without postoperative complications. A combination of vasopressors and fluid resuscitation less than 5.5 L should be used to maintain perfusion and reduce post-operative complication rates.
Tracheostomy
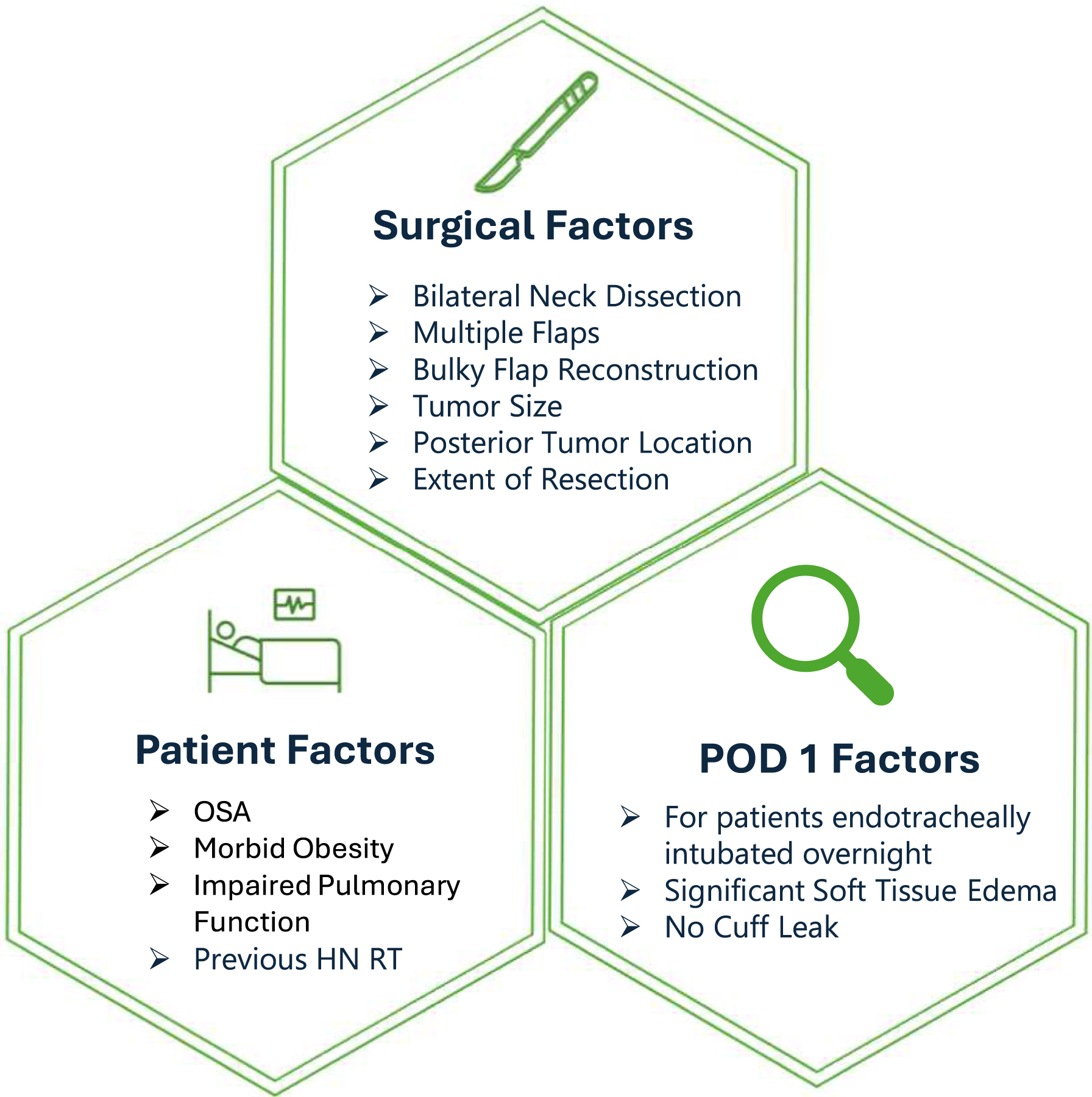
Elective tracheostomy is frequently performed in head and neck microvascular reconstruction for post-operative airway management. Overnight tracheal intubation in selected patients has resulted in an overall shorter LOS without an increase in adverse events. , A variety of scoring metrics have been developed to pre-operatively assess patients’ need for a tracheostomy. Surgical risk factors for tracheostomy include bilateral neck dissection, multiple free flaps, tumor site (eg, posterior oropharynx), extent of resection and reconstruction, soft tissue edema, and flap bulkiness. Other patient factors include previous radiotherapy to the head and neck, obstructive sleep apnea, obesity, and reduced pulmonary function ( Fig. 3 ). , , The use of a cuffless tracheostomy tube, placed at the end of the case, is preferred over a cuffed tube as the former has been shown to decrease time to decannulation and LOS by 2 days without increasing adverse events or 30-day respiratory complications. For patients not receiving a tracheostomy, extubation should be considered at the end of the case or on post-operative day one. Tracheostomy avoidance for patients undergoing complex head and neck cancer ablation and reconstruction has also become increasingly accepted with appropriate patient selection. By tailoring airway management for specific defects and reconstructions, post-operative recovery can be even further enhanced.
Post-operative interventions
Post-operative Nausea and Vomiting Prophylaxis
Nausea and vomiting are common post-operative complications that can be modulated intra-operatively. Patient-specific risk factors for post-operative nausea and vomiting (PONV) include female sex, history of PONV or motion sickness, non-smoker, and younger age, , while the duration of anesthesia and opioid use represent risk factors that can be mitigated through reduced use. , Routine use of two anti-emetics in patients with up to two risk factors and 3 to 4 anti-emetics in patients with greater than 2 risk factors is standard. , Breakthrough nausea should use rescue anti-emetics from a different class of medication as the prophylactic drugs. An example of such a regimen would be the intraoperative use of a dopamine D2 antagonist such as haloperidol and serotonin 5-HT2 antagonist such as ondansetron with an antihistamine H1 receptor antagonist such as promethazine for breakthrough nausea. Furthermore, IV acetaminophen can be used to reduce post-operative nausea and can be combined with multimodal analgesia. , , Corticosteroids such as dexamethasone have shown effectiveness in reducing PONVs in head and neck surgeries; however, they should be used cautiously in patients requiring insulin as dexamethasone substantially increased insulin needs.
Flap Monitoring
Current free flap success rates range from 90% to 95%. With 5% to 7% of head and neck free flaps requiring exploration for failure and the time-sensitive nature of free flap salvage, close monitoring of free flaps in the first 48 to 72 hours remains critical. , Clinical monitoring, through the observation of flap skin color, surface temperature, quality of bleeding with pinprick, and capillary refill time, augmented with acoustic handheld doppler (AHD) to assess intravascular arterial and venous blood flow is the current standard due to its non-invasive nature, low cost, and rapid assessment. In patients with higher Fitzpatrick skin type, muscle-only or buried flaps, clinical monitoring may be less reliable. , An externalized skin segment, if feasible, can be used to increase the reliability of clinical monitoring. ,
The most studied alternative methods are the implantable doppler (Cook Swartz) and tissue oximetry, with both demonstrating an earlier time to identification of microvascular compromise and a higher true positive rate. , Implantable dopplers have reported the highest positive predictive value for vascular compromise of all techniques assessed, and studies that have only examined head and neck specific flaps report similar values. , Furthermore, implantable dopplers in arterial systems have shown a reduction in false positives and risk of signal loss. While clinical monitoring with AHD continues to be a commonly used reliable method due to its low cost, implantable doppler is a reliable adjunct to assess monitor free flap failure in head and neck surgical patients. ,
Antithrombotics
Venus and arterial clots are the most common causes of flap failure. Pharmacologic prophylaxis with anticoagulants, antiplatelets, and thrombolytics have been administered to attempt to decrease the risk of free flap failure. In a systematic review with over 2000 head and neck free flap patients and a retrospective review with over 800 head and neck free flap patients, the routine use of antithrombotics post-head and neck reconstructive surgery was associated with an increased rate of hematoma formation and bleeding requiring intervention. A recent observational study showed that unfractionated heparin less than 500 IU/hr, or aspirin used less than 72 hours post-operatively can decrease thrombosis rates. However, this result was not able to be consistently reproduced across different studies, and often if a difference in thrombosis rates was found, it was not statistically significant. , The risks of antithrombotic use are well established, and its routine use should be avoided.
The use of antithrombotics ought to be considered in patients with increased risk for thromboembolism, such as those with a Caprini score equal to or greater than 7, or clotting disorders such as Factor V Leiden, or a CHA 2 DS 2 VASc score greater than 5. , Successful thrombolysis through the use of tissue plasminogen activators (tPA) with and without multiagent antiplatelet/anticoagulation therapy has been reported in cases of head and neck free flap salvage surgery due to vascular compromise. However, the continued use of antiplatelets, anticoagulants, and thrombolytics post anastomosis revision has been found not to impact free flap survival outcomes in head and neck surgery.
Post-Operative Pain Control
Multimodal pain control through the use of acetaminophen, NSAIDs, and gabapentin can reduce the need for post-operative opioid analgesia. , Incorporating non-opioid medication into post-operative standardized order sets, and involving PACU nurses to reinforce this regimen can be key to decreasing opioid use. Furthermore, the use of acetaminophen and adequate pain control can reduce post-operative nausea and the risk of vomiting. In patients with inadequate pain control, patient-controlled analgesia or the addition of opioids can be considered. , In cases where opioids need to be used, reduction of default pill counts in order sets is shown to reduce total prescribed MMEs.
Over a third of patients undergoing head and neck free flap surgery take opioid medication 4 months after surgery with one in every 5 opioid naïve patients chronically using opioids post-operatively. At such high prevalence rates, the implementation of a transitional pain service (TPS) in addition to multimodal pain control may be warranted. TPS implementation at Toronto General Hospital reduced opioid consumption by 69% and 44% for opioid-naïve and opioid-experienced patients, respectively, with 46% and 26% of patients weaned completely. Reduction of opioid use was also seen when TPS was implemented post-primary total joint arthroplasty and confirmed in a randomized control trial of 196 patients. , Larger scale studies within the head and neck free flap surgery population are needed to obtain a more comprehensive understanding of TPS implementation but ought to be considered for head and neck free flap patients.
Early Mobilization
Prolonged (>24 hours) time to mobilization is associated with overall complication rates, and is a significant predictor of major complications such as pneumonia, pulmonary embolism, or deep vein thrombosis (Clavien-Dindo grade IIIb-V). Implementation of early mobilization can be difficult in head and neck free flap patients due to lower limb wounds from free flaps and skin grafts. Applying a self-adhering pressure bandage, surgical boot, or cast to the flap donor sites can allow for ambulation on post-op day 1 (POD 1), though is not required. , , Despite some of these common concerns surrounding early ambulation in patients with complex lower extremity wounds, early weight bearing in patients undergoing fibula free flaps has shown significant benefits. More specifically, early weight bearing on POD 1 has been shown to be associated with shorter LOS, increased rate of discharge to home, and decreased donor-site complications.
A variety of ambulation goals,such as mobilizing from bed to chair , , or a step count, have been implemented in ERAS protocols. The use of a pedometer to measure step counts allows an accurate measurement of a patient’s daily mobility and may also lead to future standardization of post-operative ambulation goals. , Two common strategies to increase post-operative early mobilization compliance rates include the education of staff on new ambulation goals and the utilization of standardized order sets with physical and occupational therapy consults on POD 1. , ,
Post-Operative Nutrition
Head and neck cancer patients already face a high burden of malnutrition and sarcopenia. Early post-operative nutritional intervention has been shown to prevent weight loss in head and neck cancer patients, a major risk factor for post-operative complications like pharyngocutaneous fistulas, flap failure, and wound necrosis. A prospective cohort study by Kerawala and colleagues analyzed 200 patients undergoing head and neck free flap reconstructive surgery and showed that early (<24–48 hours) post-operative enteral feeds led to decreased length of hospitalization without an increase in complications. , Free jejunal reconstruction, history of gastroesophageal surgery, and a prognostic nutritional index have been shown to be risk factors for difficulty with early enteral nutrition. , , , Post-operative ileus and intraoperative blood loss are complications that can occur after such a procedure that could further discourage early enteral feeding. Magnesium oxide and mosapride citrate could be used in patients undergoing free flap reconstruction to promote gastrointestinal motility.
Post-operative Level of Care
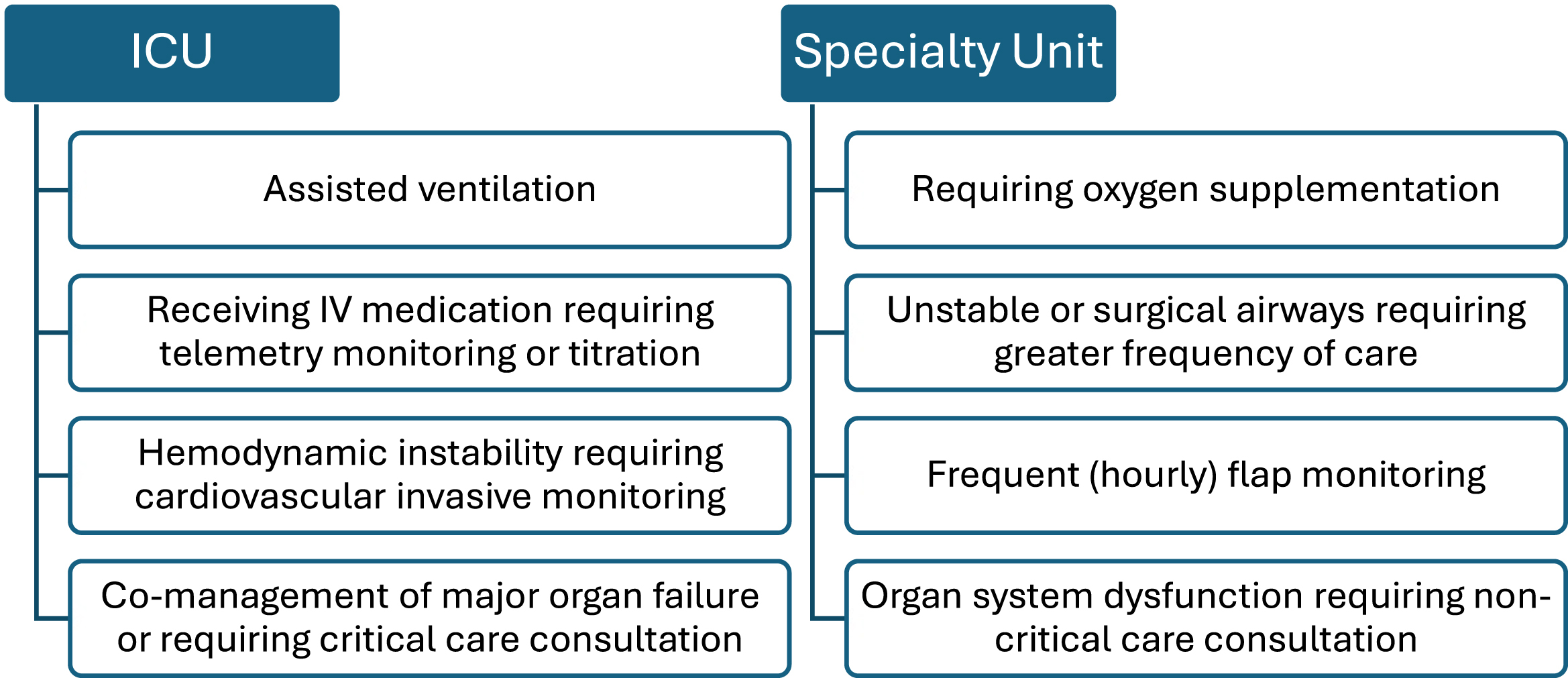
Routine admission to the intensive care unit (ICU) increases the length of hospitalization without decreasing the complication rate. , Post-operative head and neck free flap patients require multidisciplinary care with frequent observational and maintenance needs including flap checks and tracheostomy care. These care demands–with staffing requirements to match patient needs–may be found in dedicated high-dependency units or intermediate care wards ( Fig. 4 ). The de-escalation of level of care in head and neck cancer patients has been a key indicator of success in recent implementations of the ERAS protocol. Patients requiring advanced respiratory support, support of 2 or more organ systems, or those with chronic impairment of one or more organ systems that restrict daily activities are likely appropriate for ICU level care.
Related posts:
 Microvascular Free Flap Practice Management and Career Development
Updates in Assisted Advanced Technology for Microvascular Free Tissue Transfer in Head and Neck Surgery
Contemporary Approaches to Head and Neck Reconstruction
Free Flap Reconstruction of the Oropharynx
Microvascular Free Flap Practice Management and Career Development
Updates in Assisted Advanced Technology for Microvascular Free Tissue Transfer in Head and Neck Surgery
Contemporary Approaches to Head and Neck Reconstruction
Free Flap Reconstruction of the Oropharynx
 Advances in Midface Reconstruction
Advances in Midface Reconstruction
 Custom Craniofacial Implants
Custom Craniofacial Implants
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


