Free Anterolateral Thigh Flap
John R. Lien
Kevin C. Chung
DEFINITION
The anterolateral thigh flap is a versatile free flap that is often harvested as a fasciocutaneous flap, supplied by the descending branch of the lateral femoral circumflex artery (LFCA).
It can be harvested also as a cutaneous or musculocutaneous flap with the vastus lateralis, with the option of an innervated flap with inclusion of the lateral femoral cutaneous nerve (LFCN).
ANATOMY
The LFCA arises from the profunda femoris artery and divides into three branches (ascending, transverse, descending) deep to the sartorius and rectus femoris muscles (FIG 1).
The descending branch of the LFCA courses distally along the medial border of the vastus lateralis, supplying perforators of the anterolateral thigh.
Perforators supplying the anterolateral thigh are either of the following:
Musculocutaneous, which pass through the vastus lateralis muscle
Septocutaneous, which travel along the septum between the vastus lateralis and rectus femoris
The LFCN passes under the inguinal ligament and pierces the deep fascia to innervate the skin of the anterolateral thigh.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients with a history of peripheral vascular disease, active nicotine use, or generally poor health are not candidates for free tissue transfer.
Obese patients may have a very thick flap and require primary thinning or secondary debulking procedures.
Examine the donor site for scarring and obtain a thorough history to include previous injury or surgery to the thigh.
We do not routinely obtain preoperative angiography.
SURGICAL MANAGEMENT
Anterolateral thigh flap is indicated for large soft tissue defects, though it is versatile and can be used for smaller defects if needed.
A two-team approach can be used to decrease surgical time.
Flap vascular pedicle can be long (12 cm), allowing for anastomosis outside of zone of injury, if necessary.
Flap dimensions are generally limited to 35 cm long and 15 cm wide on a single dominant perforator, though multiple perforators are preferred in large flaps.
Limiting the width of the flap to 8 cm generally permits primary donor-site closure.
Preoperative Planning
Preoperative Doppler exam is used to confirm the presence of a perforator.
If one is not detectable, consider the contralateral thigh or a different type of flap.
Positioning
Supine with a bump under the right hemipelvis, or lateral decubitus position
Drape out the entire lower limb for leg manipulation.
Ensure the anterior superior iliac spine (ASIS) and patella are included in the operative field.
Approach
A suprafascial approach to flap harvest achieves a thinner flap design, though it is more technically challenging.
Subfascial flap harvest is technically easier to identify the vascular anatomy but will result in a bulkier flap.
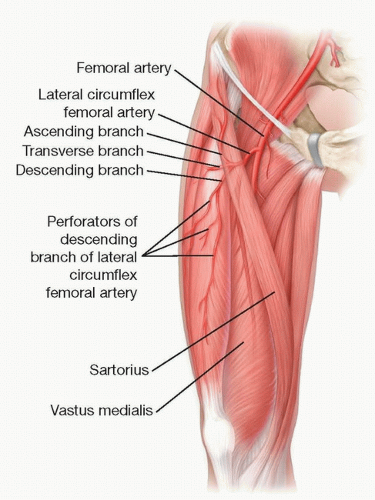 FIG 1 • Anterolateral thigh flap anatomy. |
TECHNIQUES
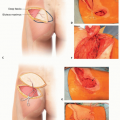
▪ Flap Design
Draw a line from the anterosuperior iliac spine (ASIS) to the superolateral border of the patella. This represents the intermuscular septum between the rectus femoris and vastus lateralis muscles (TECH FIG 1).
Use a portable Doppler device to identify the perforator around the midpoint of this line.
80% of perforators are found within 3 cm of this point.1Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree