CHAPTER 24 Form Stable Shaped High Cohesive Gel Implants

Summary/Key Points
Introduction
With the introduction of shaped textured implants surgeons started to think in terms of shape and dimensions rather than volume and cup size.1 In order to fully exploit the opportunity for creation of a natural breast shape offered by the shaped devices, careful attention must be given to the surgical techniques of pocket dissection and implant placement for shaped devices.2–5
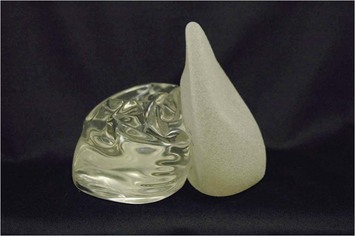
In the last decade much of the discussions in the plastic surgery literature has focused on the difference between shaped and round implants, however, a much greater divergence relates to the use of form stable versus non-form stable implants (Fig. 24.1). Basically most aspects of such breast augmentations are different. The way of selecting implants is different. Patient preoperative markings, surgical techniques and postoperative recommendations and results also differ. These are not just new type implants, they represent a new concept in breast augmentation surgery. Surgeons who believe that form stable implants behave in the same way as non-form stable implants will tend to plan, select implants and perform surgery in traditional ways. Unfortunately, they are bound to encounter significantly more complications and problems.
Patient and Implant Selection
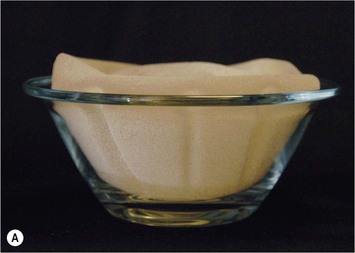
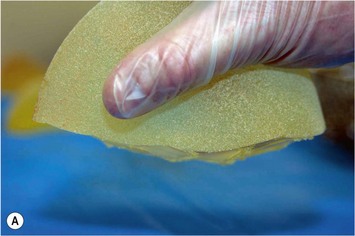
Ever since silicone breast implants were introduced in the early 1960s implant selection has been a relatively arbitrary process where the surgeon has estimated the volume of the implant in relation to patients’ desires and biological prerequisites based on his own experience. As form stable implants cannot be deformed (Fig. 24.2) dimensional planning and implant selection is necessary. Instead of estimating an appropriate volume the ideal dimensions of the implant are calculated.

Definition of Patient Desires
The general information about breast augmentation surgery can be conveyed in many different ways and well educated patient coordinators and/or in the written form and a patient information book have proved extremely useful.28 A full size mirror in the doctor’s office is also an extremely important part of the consultation process as the dimension and proportions of the expected result can be demonstrated for the patient by displacing the breast medially and laterally, showing expected borders of the new breast and showing projection of different implants. To use sizers in a sports bra should not be part of the consultation in the first stages but final testing with suitable sizer in a sports bra can be a good way to create final trust in the implant selection for the patient.
Examination of the Breast Tissue and its Envelope
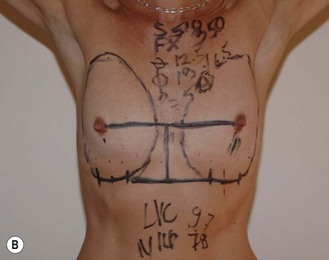
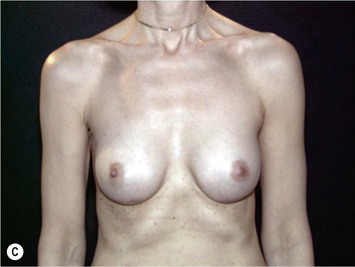
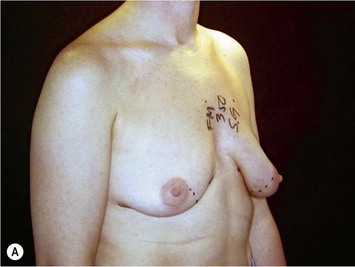
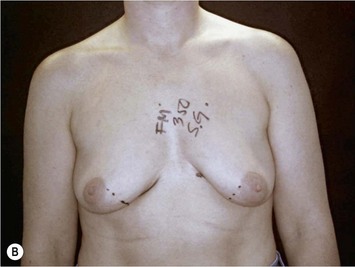
As breast asymmetries are extremely common but not always noted by patients, these smaller asymmetries should be noted and pointed out to the patient. The characteristics and distribution of the glandular tissue should be examined as it has implications on implant selection. A patient with a dense, relatively constricted gland and short nipple inframammary fold distance has increased risk for a double bubble deformity in the lower pole and they may do better with a more projecting implant and shorter implant heights. The surgeon may also need to modify the gland with scoring or unfolding of a glandular flap.6 When selecting implants it is also very important to consider the envelope’s characteristics. A lax envelope may need more implant projection to fill it. A simplified way of estimating envelope laxity is to do an anterior pull stretch test (APSS) according to the TEPID-system.7 By grabbing the areola tissue beside the nipple and pulling firmly (warn the patient before doing this procedure as it may be uncomfortable), the extensibility of the envelope can be measured. This will provide information on suitable implant projection. An alternative to this is to measure the nipple–inframammary fold distance on the relaxed tissue and maximum stretch and put this in relation to implant dimension (see LVC and N-ILP measurements below). Obviously the selected implant has to suit the characteristics of the gland and envelope in accordance with all tissue based planning systems.7,8 However, it should also be remembered that patient desires must be considered and for a patient with relatively lax tissue who desires a small augmentation, but needs a larger implant to fill the envelope an alternative is to combine a small augmentation with a mastopexy, which both takes patient desires and the envelope characteristics into consideration. Also, patients with very tight tissue could be treated with more projecting implants than the anterior pull test indicates as the tissue will expand over time (Fig. 24.3).

Operative Technique I: Selection of Adequate Implant Dimensions
Selection of ideal implant width
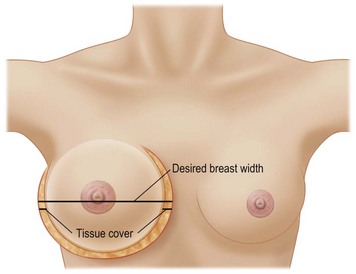
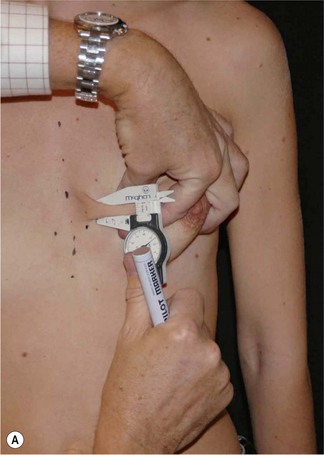
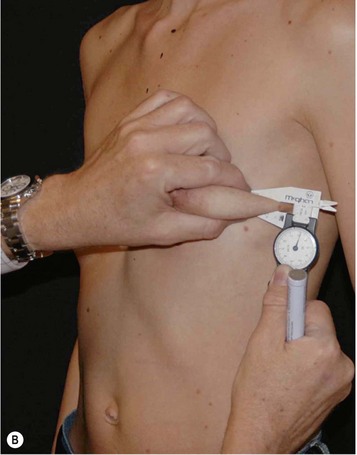
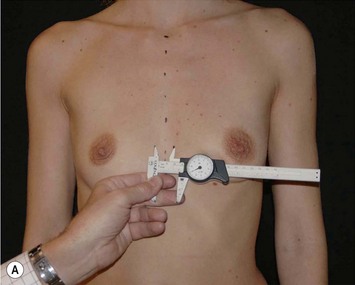
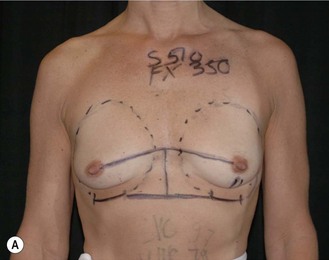
Having communicated with the patient and examined the biological prerequisites, the next step is the definition of the ideal implant dimension. The first and most important part of this is to define the ideal implant width. This is equal to the desired breast width minus the tissue cover on the implant (Fig. 24.4). Thus the medial and lateral thickness of tissue has to be examined. This is done at the height of the nipple–areola complex at the expected inner and lateral border of the implant (Fig. 24.5). Tissue cover is measured with a pinch and as a pinch of tissue is a double fold of skin and subcutaneous tissue, the measurement in the medial and lateral part of the breast should be divided by two when subtracting this number from the desired breast width. The desired breast width usually should leave an intermammary distance between 2 and 3 cm and the lateral protrusion of the breast should respect the anterior axillary line (Fig. 24.6). The distance between these two points can be measured with a caliper and the tissue cover, as mentioned according to the description above, is then subtracted for information about ideal implant width. The existing breast width should also be measured as implant selections that are considerably wider than the existing breast width should be avoided as it increases the risk for complications such as palpability and visibility of the implant.

Selection of implant height
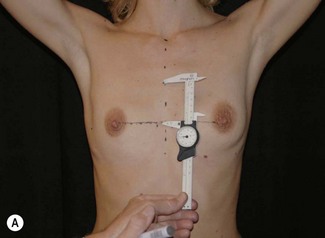
Having defined and communicated ideal implant width with the patient, the next step is to recommend a suitable implant height. It should be remembered that preoperative upper and lower pole appearance is of great importance for the implant height selection. For example, bulging upper thoraxes may be exaggerated by selection of full height implants whereas depressions in the upper thorax more favorably could be treated with full height implants. When selecting implant height it is important to measure and localize where the lower and upper pole of different implants will be located and compare this to how the upper pole shape is estimated to appear and how the implant correlates to the existing submammary fold and the lower pole appearance of the breast (Fig. 24.8). To be able to estimate where the upper and lower pole of different implants will be located during the consultation, the patient is asked to put her hands on top of her head. This 45° elevation of the arms above the horizontal plane is an accurate estimation of where the nipples will be positioned after a proportionate breast augmentation (see preoperative markings below). Knowing ideal implant width the height of different implants can easily be looked up in the manufacturers’ charts. Usually half of the implant height should be positioned above the nipple–areola complex after the augmentation and half below. Thus it is easy to measure above and below the nipple with the arms on top of the head to estimate how the upper and lower poles of the breast will appear with different implant heights.

Selection of adequate implant projection
This recommendation of the ideal footprint (height and width) or base plate of the implant obviously has no volume as it is only two-dimensional. The projection, the third dimension of the implant, will provide the final volume of the implant. Implant projection is highly dependent on patient desires, but remember to consider the envelope characteristics as loose envelopes may need more projection or a mastopexy. Also, patients with a contracted lower pole may have less risk for double bubble deformity if more projecting implants, for instance Allergan Style 510, are selected (Fig. 24.7). A good way of selecting implant projection is to communicate this with the patient standing in front of the mirror.


Indications
Form stable breast implants are considered more demanding and difficult to use. An obvious question is then why is there a need for them. The answer to this question is that form stable implants control the shape of the breast in a much better way, especially if we consider long-term effects of a breast augmentation. The high cohesive silicone gel breast implant retains its shape even if it is cut into two pieces and even if it is put under pressure (Fig. 24.9). On the other hand, relatively small forces are needed to deform a responsive low cohesive silicone gel implant. The clinical consequence of this is that a low cohesive silicone gel implant easily is deformed into a spherical shape during capsular contraction (Fig. 24.10). Contrary to this, capsular contraction on high cohesive silicone gel implants deforms implants much less. Clinically, this difference has been observed by the author in a number of cases. A textured shaped form stable implant should also be positioned into a snug fitting implant pocket and one implication of this is that it moves less in the cranial direction during capsular contraction compared to a round smooth implant which usually is massaged to retain a large implant pocket and softness. Thus circumferential shrinkage during capsular contracture moves a smooth walled implant in a large pocket more in the cranial direction (Fig. 24.11). Consequently, these benefits of form stable implants have improved the appearance and the control of the breast shape better and long-term follow up (>10 years) indicates good stability of results (Fig. 24.12). The use of shaped form stable implants constitutes a new era in breast augmentation surgery: The era of breast shaping and long-term customized control of breast shape versus the traditional breast volumetric filling or stuffing era. Obviously a prerequisite for controlled shaping of the breast is not only to have a form stable shaped implant, but also a wide variety of different implant shapes.










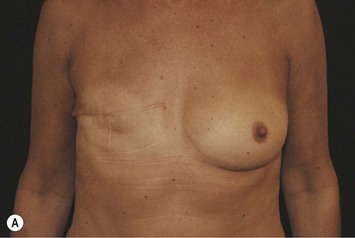
Other advantages relating to these devices have been reviewed elsewhere.9 Among these are that breast augmentation can be more customized than ever before and that the great variability of different implant shapes makes it possible to compensate for breast asymmetries. This is also a great advantage when it comes to breast reconstructive procedures where bilateral treatment with different sized implants (Fig. 24.13) and different shaped implants can provide a long-term stability of the results compared to unilateral implantation of a round, non-form stable device.10 High cohesive silicone gel also minimizes gel bleeding and leakage after a shell rupture and as the filler is form stable, irregularities such as fold and rippling are significantly less common.11 Capsular contracture rates have also been lower for form stable implants compared to implants filled with saline or regular low cohesive silicone gel.12 It is also likely that the form stable filler minimizes the envelope movements, and thus the wear of the envelope, giving better chances of low long-term risk for ruptures. This has also been clinically proven in long-term magnetic resonance imaging (MRI) evaluation of these devices.13 The rupture frequency has been as low as 0.3% after up to 9 years of implantation, and comparing this to other similar MRI studies on non-form stable breast implants these have shown that the risk for rupture has been considerably (3.5–17%) higher.14–17 Others have also confirmed the low rupture of Allergan form stable implants whereas other manufacturers’ form stable implants have not been confirmed to have this low incidence of ruptures.18,19

In spite of all these advantages several surgeons refrain from use of form stable implants. A common argument against is that patients are happy with the non-form stable devices provided. This is true as patients usually are happy even with inferior result, but this is no reason why we should refrain from doing our best to improve results. It is also claimed that non-form stable implants deform into an ‘anatomical’ shape when a patient is standing,20 which also is true if the device is underfilled with a low cohesive filler and if there is no capsular contraction (Fig. 24.14). However, during capsular contraction the implants become more round and artificial in their appearance (Fig. 24.10) and also the shaped ‘deformity’ of a round implant increase rippling and irregularities in the upper pole which is likely to increase the wear of the envelope. It is sometimes also claimed that form stable implants behave unnaturally on the chest wall giving unnatural appearance when the patient is lying on their back. This has not been our clinical experience as even these implants move laterally when the patient is lying on her back. The firmness and movement of the implant is more related to common and small degrees of capsular contraction not regarded as true Baker II deformities. These small degrees of capsular activity usually regarded as natural softness are relatively common and by the author regarded to be more important for the movement and firmness of the breast than the firmness of the implant itself.







Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


