Forked Flap
D. R. MILLARD JR.
EDITORIAL COMMENT
Columellar lengthening is obtained by adding tissue from the lip. This is exemplified in an adult male who has undergone the procedure as a child and has to shave under his nose. It is not clear whether or not the patient with a bilateral cleft lip has an actual shortage of skin at the level of the columella or if everything is pulled down because of the distortion of the tissues. An alternative approach would be to stretch out the pulled down columella by a bone graft that will hold the tip of the nose up, as does the spoke of a tent.
The forked flap was initially designed to lengthen a short columella in a secondary bilateral cleft. The forked flap is taken out of the lip continuous with the present short columella. This approach not only lengthens the columella, but also allows revision of bilateral lip scars and reduces the wide prolabium to a more natural philtrum dimension (1, 2, 3, 4).
INDICATIONS
The forked-flap technique is of value in bilateral cleft patients when the columella is short and the upper lip is not tighter than the lower lip (Fig. 72.1). The procedure also has been found of value in primary bilateral cleft patients when the prolabium is extremely diminutive (Fig. 72.2), as well as when the prolabium is wide enough in the primary deformity to spare a forked flap from its sides and still leave enough central portion for a philtrum (Fig. 72.3).
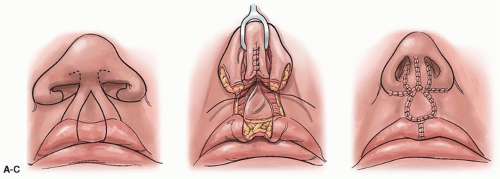 FIGURE 72.1 A: Short columella and wide prolabium. Note that the forked flaps include the old bilateral cleft lip scars. Note also that the membranous septal incision is extended over the nasal tip, as indicated by the broken line. B: The forked flaps are sutured together and advanced along the septum. They are sutured together in front and then tubed behind to create a column. The distal tips of the fork are left free to spread at the columella base. The alar bases, with their tips denuded of epithelium, are sutured together at the nasal spine in a cinching procedure. C: The ends of the forked flaps are sutured to the alar bases to form the nostril sills. The lateral lip elements are sutured to the sides of the reduced prolabium, and the lateral mucocutaneous flaps are advanced to the midline below the prolabium to create a better cupid’s bow and tubercle.
Related posts: Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Oral Mucosal Flaps for Septal Reconstruction Oral Mucosal Flaps for Septal Reconstruction
 Postauricular and Retroauricular Scalping Flap (The Paras Flap) Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|