Chapter 7 Forehead Rejuvenation
Summary
Introduction
The plastic surgery armamentarium for forehead rejuvenation has expanded considerably during the past 15 years.1–12 Whereas the focus of rejuvenation in the past was focused mainly on the face and neck, it has now become widely recognized that rejuvenation of the forehead is essential to produce a natural, well-balanced result. There is now greater emphasis on minimizing incisions and long-term side effects, such as numbness, while achieving a superior aesthetic outcome with improved patient satisfaction. Less invasive techniques have also emerged.
This chapter reviews most of the techniques available for forehead rejuvenation.
Indications
Fat injection
Subcutaneous forehead rhytidectomy
Preoperative History and Considerations
Patient assessment
A proper forehead length and eyebrow position with a smooth and properly contoured forehead is an integral part of facial beauty (see Chapter 1). Any disturbance of this balance undoubtedly detracts from the pulchritude of the face.
Patients with eyebrow and eyelid ptosis either consciously or subconsciously may recruit the frontalis muscle to aid in opening their eyelids.14 These two conditions should be differentiated in one of the following two ways:
Fat Injection
Since the introduction of fat injection as the means to eliminate facial lines, there has been a longstanding debate about its efficacy and reliability. In 1911 Brunings3 injected small cubes of autologous adipose tissue under the skin during rhinoplasty, but there was significant absorption of the injected fat.2 Interest in fat injection for facial rejuvenation has recently re-emerged as a result of the refinement of techniques and more reliable outcomes.15
Operative Approach
Relevant surgical anatomy
The anatomic layers of the forehead are both continuous and analogous to the five layers of the scalp.16 There is a gradual decrease in sebaceous gland content of the skin in a cephalad direction.
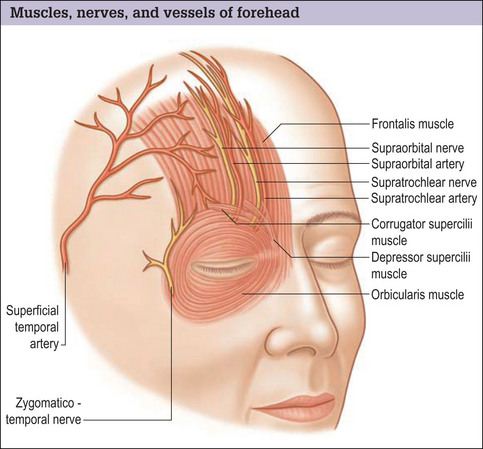
As with the scalp, the forehead skin is firmly adherent to the underlying epicranial layer. The epicranial layer is formed by the vertical fibers of the frontalis muscle anteriorly (Fig. 7.1) and the occipitalis muscle posteriorly. The galea aponeurotica spans these muscles.
Operative Technique
Complications
Fat injection is generally an uncomplicated procedure, but over- or under-injection may occur.
One serious complication of fat injection, which is extremely rare, is blindness.11,12 The loss of eyesight is probably related to embolization of the injected fat into the retinal artery. If this complication develops, immediate consultation with an ophthalmologist is necessary. Intentional overcorrection may result in longlasting glabellar fullness, which may ultimately resolve. This site is more privileged as a fat recipient site than most sites in terms of retention of the injected volume, and complete fat absorption is unlikely, which reduces the need for an overcorrection.

Fat Graft
Operative Approach
Since its introduction by Neubeur in 1893, the use of an autologous fat graft has been consistently popular.18 The degree of fat graft take is:
Operative technique
Complications
Fat graft may result in irregularities, infection, or accumulation of a small amount of blood around the graft, which may persist and cause the patient concern. These undesirable outcomes are unlikely.

Transpalpebral Corrugator Resection
Operative Approach
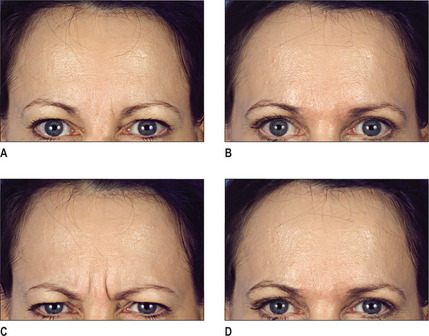
A transpalpebral incision may be used to resect the corrugator which usually results in disappearance of the frown lines (Fig. 7.4A-D).19,20 Transpalpebral corrugator resection may be performed concurrently with an endoscopic procedure to facilitate removal of the corrugator muscle. The advantages of this operation are its simplicity with direct and full exposure of nerves and muscles. The results are highly predictable and reproducible. When combined with a blepharoplasty, fat is readily available for replacement of the corrugator muscle.
Relevant surgical anatomy
Frontalis muscle
During animation, the frontalis muscle, which expresses attention, elevates the eyebrows and causes transverse wrinkling of the forehead.21 Its contraction provides a constant, cranially directed force vector on the eyebrows.
Orbicularis oculi muscle
Temporal and zygomatic branches of the facial nerve22 innervate the cephalic portion of the orbicularis oculi.
Corrugator supercilii muscle
Supraorbital and supratrochlear nerves
The supraorbital and supratrochlear nerves (see Fig. 7.1) are the terminal branches of the ophthalmic division of the trigeminal nerve (CN V) and provide sensory innervation to the forehead and scalp:
Operative technique




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


