31
Folliculitis
Superficial Folliculitis
• Common; characterized by follicular papules or pustules that are often on an erythematous base.
• Often pruritic, sometimes painful.
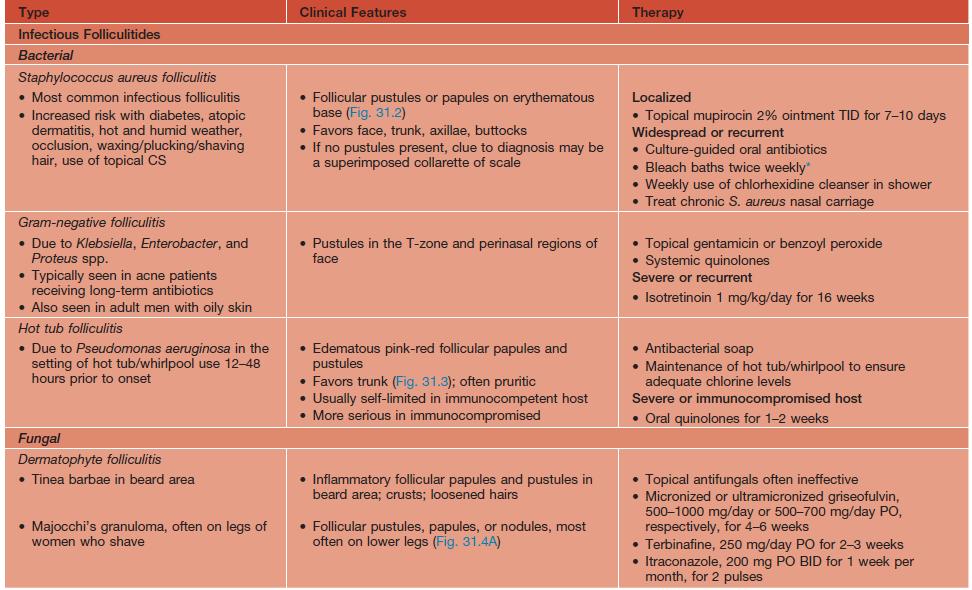
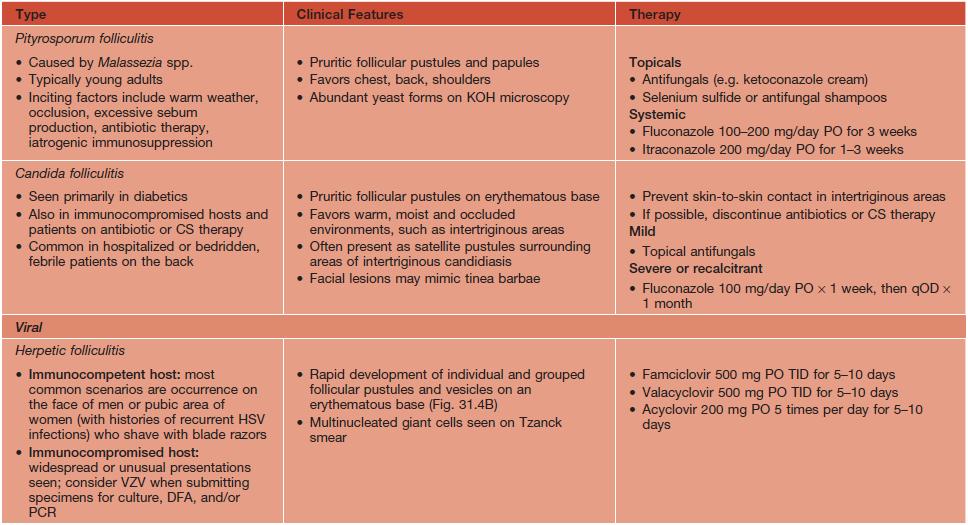
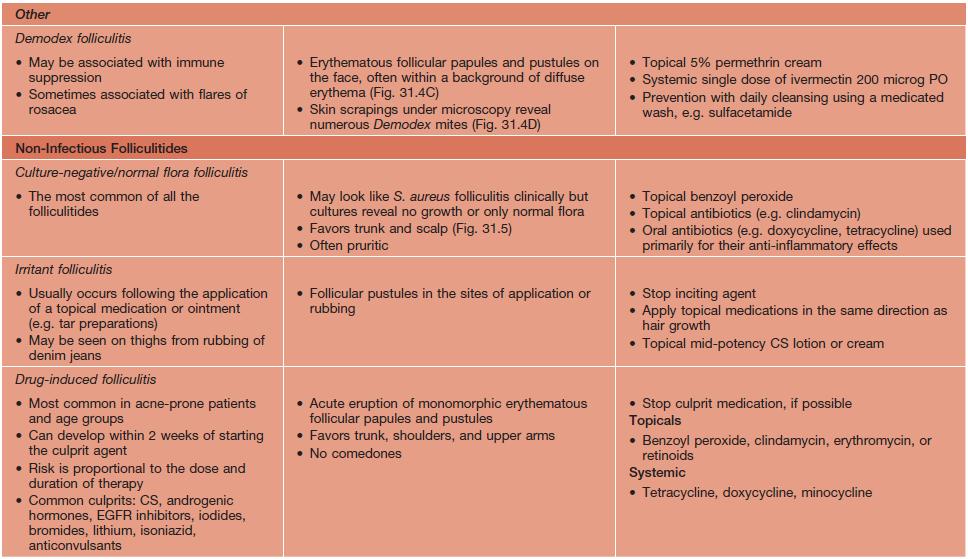
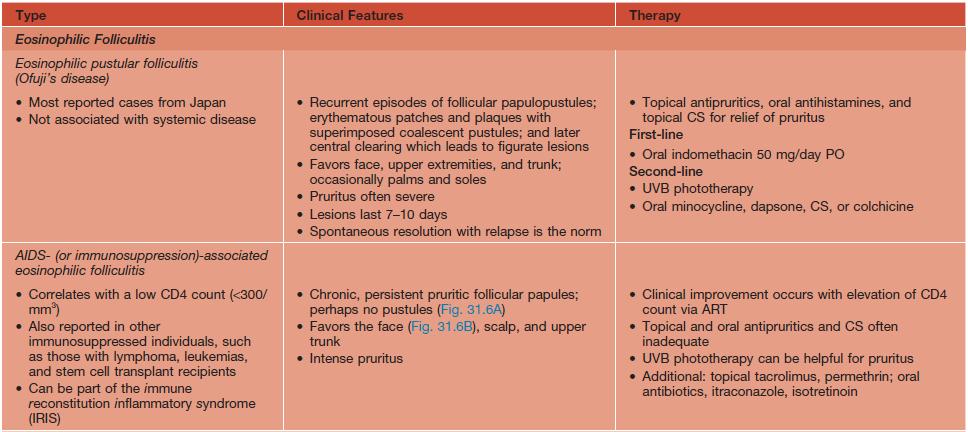
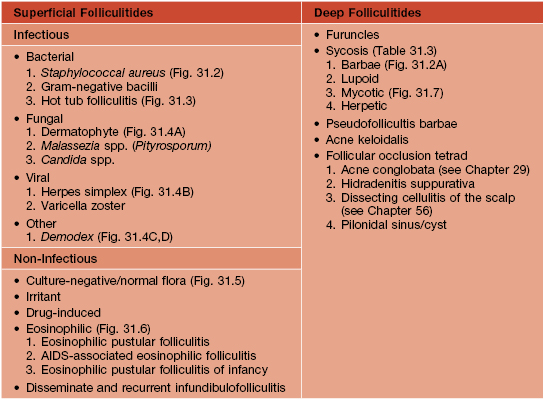
• Multiple, less common etiologies (Table 31.1), requiring a systematic approach for adequate diagnosis and treatment (Fig. 31.1; Table 31.2).
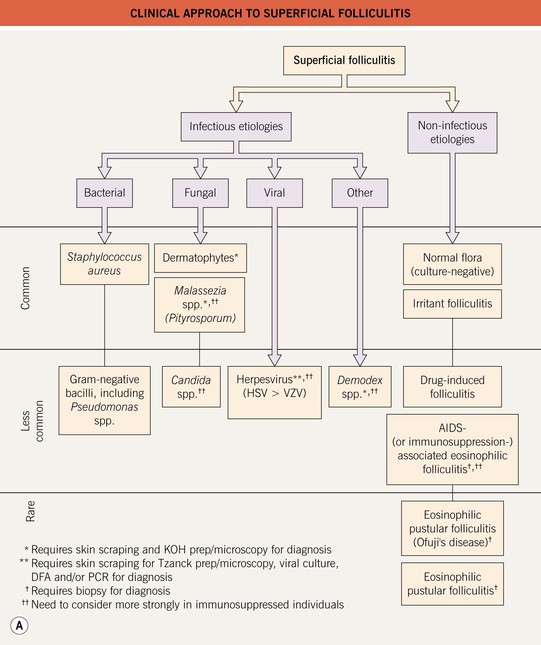
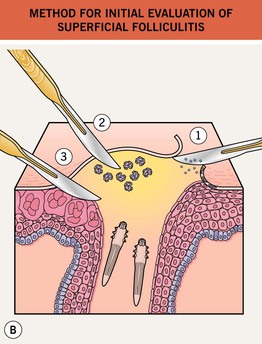
Fig. 31.1 Superficial folliculitis – clinical approach and initial evaluation. A Clinically, edematous lesions of folliculitis are most suggestive of eosinophilic folliculitis, Demodex folliculitis, and Pseudomonas ‘hot tub’ folliculitis. B If considering dermatophytes, Malassezia spp., or Candida spp., then obtain scrapings from the peripheral scale and the roof of the follicular pustule for KOH (potassium hydroxide) microscopy (1). If considering bacterial etiologies, and depending on the host, the pustular fluid should be sent for gram stain, culture, and sensitivity (2). If considering viral etiologies, the base of the unroofed lesion should be vigorously scraped in order to collect the viral-laden keratinocytes for Tzanck prep/microscopy, viral culture, DFA (direct fluorescent antibody), and/or PCR (polymerase chain reaction) (3). Likewise, if considering Demodex folliculitis, scrape the base of the lesion vigorously for KOH microscopy (3) (see Fig. 31.4D).