52B Follicular Unit Excision Terminology And Overview
Summary
Keywords: FUE terminology FUE devices FUE quality control measures graft damage categories transection classification FUE history follicular unit extraction follicular unit excision
Key Points
•A lack of published scientific evidence in the hair restoration field, and reliance on the experience of well-practiced physicians, may make it difficult for new or less experienced surgeons to familiarize themselves with concepts and procedures.
•This chapter aims to summarize the work of the International Society of Hair Restoration Surgery (ISHRS) to standardize follicular unit excision (FUE) terminology and encourage consistent and effective communication within the field worldwide.
•Common standards for measurement of quality in FUE procedures are defined.
52B.1 Introduction
52B.1.1 Follicular Unit Excision History and the Need for Terminology
Follicular unit excision (FUE) can be dated back to the 1930s. Dr. Shoji Okuda, a Japanese physician, invented the first rudimentary form of FUE. Within his research, he focused on using full-thickness grafts on hairless areas such as the scalp, upper lip, and eyebrows. The discovery of FUE, however, was lost in translation as it was not until Dr. Yoshihiro Imagawa translated Dr. Okuda’s published work into English many decades later that it was incorporated into the western publications.1 The use of a 1-mm needle for FUE was first described by Dr. Masumi Inaba in 1988, while Dr. Woods in Australia successfully began performing FUE in 1989 and was the first to successfully demonstrate scalp hair growth with body hair transplants. Drs. Rassman, Bernstein, Harris, True, and Cole have all contributed to the development of FUE techniques and devices.2 Many new devices and techniques continue to develop. These are presented throughout the chapters of this section of the textbook.
The International Society for Hair Restoration Surgery (ISHRS) created the FUE Research Committee to encourage research and address the issues surrounding FUE and its rapid development. As with any field, consistent, agreed-upon, and accurate terminology and definitions are important for concerns. To this purpose, the FUE Terminology Subcommittee was created and a working document produced in hopes that standard terminology would allow for effective communication. This chapter is a product of the work of this committee and much has been published elsewhere.3,4,5,6
52B.2 Anatomical and Histological Terms
Follicular units ( Fig. 52B.1): These units can have two to four terminal follicles and one or, rarely, two vellus follicles, the associated sebaceous lobules, and the insertions of the arrector pili muscles of the terminal follicles.7 Follicular canals and vellus follicles of follicular units may be joined or remain separate. Two- or three-hair shafts may be seen in a single canal (at the level of the infundibulum).
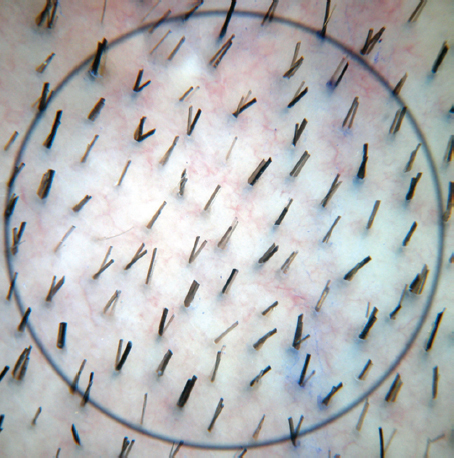
Fig. 52B.1 Follicular unit.
Follicular families, follicular groups, or follicular clusters ( Fig. 52B.2): Scalp hair can be found in distinct clusters that can consist of one or more follicular units. These clusters are found in close proximity to each other when exiting the skin. It can be difficult in complex donor areas to distinguish between individual follicular clusters as complex donor areas may contain closely aligned or many large bundles.6
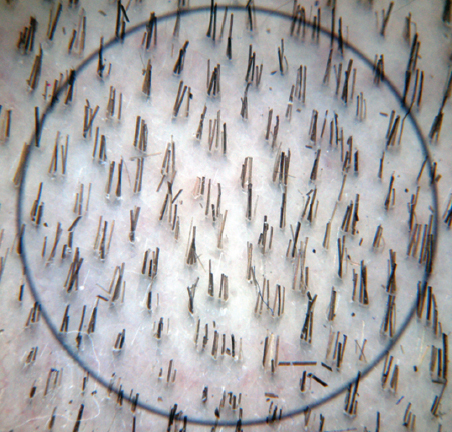
Fig. 52B.2 Follicular cluster.
Infundibulum of the hair shaft ( Fig. 52B.3 a): This is the upper segment and extends from the epidermis level to the entrance of the sebaceous gland. Infundibulum cells can aid in the regeneration of the epidermis if injury occurs.
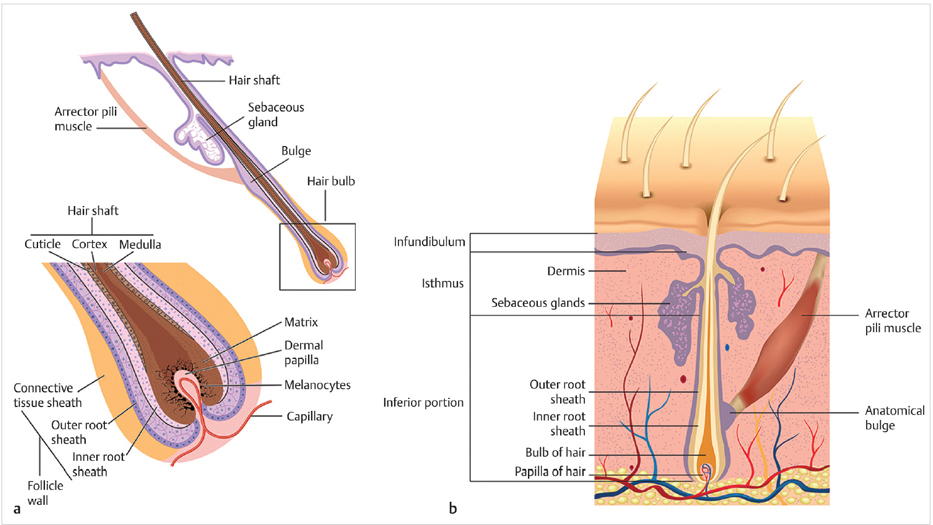
Fig. 52B.3 (a) Anatomy of a hair follicle. (b) Layers of a hair follicle.
•Bulge area cells: These cells are multipotent epithelial stem cells. This area is easiest to see when the hair follicle is in the telogen phase and most difficult to identify in mature anagen hair follicles.
Inferior portion of the hair shaft: This is the lowest segment and extends from the insertion of the arrector pili muscle to the base of the follicle. At the base of the follicle is the bulb.
•Bulb ( Fig. 52B.3b ): This is the location of matrix keratinocytes, which are responsible for hair shaft growth.
•Dermal papilla (DP): The hair bulb surrounds the mesenchyme-derived cells, which contribute to hair follicle formation and the hair cycle as the site of growth factors.8
•Connective tissue sheath (CTS): This is the outermost layer of a hair follicle and contains elastic filaments that give the intact follicle support. This connective tissue can help increase graft survival if harvested along with the follicular unit.
•Outer root sheath (ORS): The CTS surrounds the ORS, which is continuous with the epidermis.
•Inner root sheath (IRS): The ORS encloses the IRS and is made up of three cell layers that protect and surround the hair follicle and may serve as a frame for a growing hair shaft.6
Follicle depth ( Fig. 52B.4): The distance between the skin surface and the full length of the follicle can vary. The angle at which follicles enter the scalp is not necessarily the direction that follicles assume as they extend into adipose tissue.

Fig. 52B.4 Follicle depth.
Follicle curve ( Fig. 52B.5) or curl ( Fig. 52B.6): It is common to have this in natural curly-haired individuals. A follicle curl can be soft, medium, or hard and can be prone to transection when a straight punch is used to harvest. Large punches (1.0–1.2 mm), blunt punches, and hypodermic needs can help assist when harvesting very curly hair.

Fig. 52B.5 Follicle curve.

Fig. 52B.6 Follicle curl.
Splay ( Fig. 52B.7 a): This is when a follicle (or all follicles) within a follicular cluster that diverges away from adjacent follicles. Splay typically occurs in the lower portion (lower one-third) of the follicular unit and can vary in degree.6
•Structural splay and iatrogenic splay ( Fig. 52B.7 b): Dr. True has recently introduced this concept of structural splay which exists anatomically in the tissue. Iatrogenic splay is produced by the method of FUE. FUE techniques in which the punch is inserted superficially may often produce extreme splay of the bulb portion of the follicles as a consequence of stripping away the perifollicular tissue during the extraction phase of excision. Such grafts are very difficult to place with forceps and are more amenable to implanter placement.
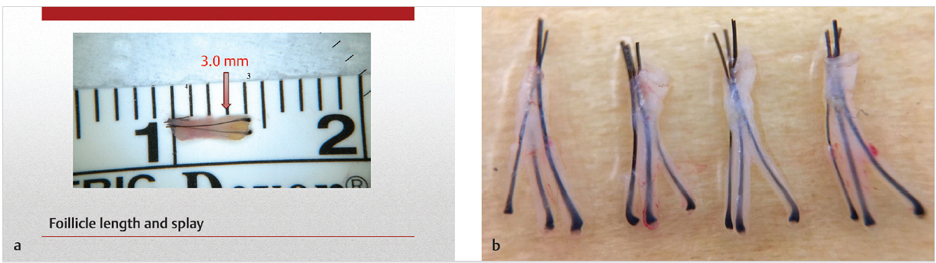
Fig. 52B.7 (a) Structural splay. (b)Iatrogenic splay.
•Tethering: The attachment of the CTS to the ORS is also used to help maintain follicular group position. Tethering strength can vary between individuals and is usually pretty weak. However, stronger tethering will require more tension when extracting the follicle.6
52B.3 Donor Area–Related Terms
Safe donor area: This is considered the portion of the scalp that contains “permanent hair” that is suitable to be used in hair restoration procedures. The term “permanent” is used loosely, as it can be challenging to predict future hair loss and there are no guarantees that all grafts from this area will be permanent. The safe donor area is usually centered in the occipital protuberance, approximately 2 cm above the superior helix of the ear. This approximation as the safe donor area relies on many factors and the experience of the hair transplant surgeon. Each patient is different and it may be particularly difficult to determine the safe donor area in younger patients.4,6
Donor area templates ( Fig. 52B.8): These can be used to demarcate the safe donor area margins and divide this area into excision zones to assist in determining the number of follicles that can be safely excised.
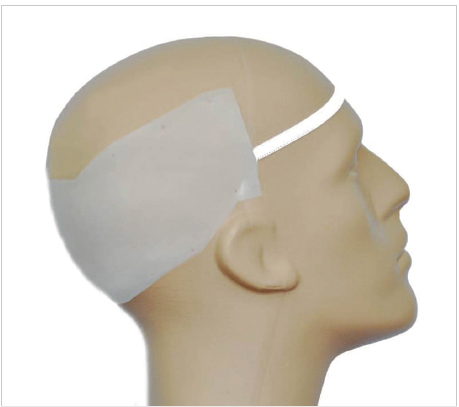
Fig. 52B.8 Donor area templates.
Donor area regions ( Fig. 52B.9): The safe donor area can be divided into zones where it is safe to harvest follicles.
•Major regions: The occipital and temporal regions of the safe donor area are commonly referred to as major regions.
•Minor regions: Zones that are used for secondary use (e.g., nape, areas inferior to major regions) are referred to as minor regions and can be designated in individuals without extensive hair loss. Hair in these regions, however, is less often considered safe and is finer and/or more often is in the telogen phase.
•Additional donor regions: These regions can also include the temporal areas located in front of the ears, the supra-auricular areas, and the lateral humps.4,6
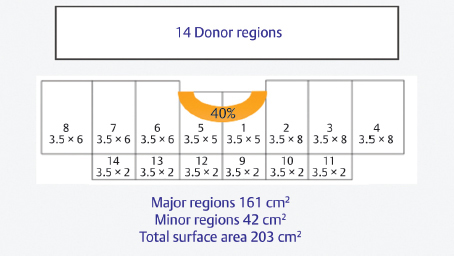
Fig. 52B.9 Donor area regions.
Donor area hypopigmentation ( Fig. 52B.10): This is loss of skin color in the donor area. This can occur through the loss of melanin, loss of follicle hue, and loss of circulation during the healing process. Hypopigmentation manifests as white dot-shaped marks. The size and shape of these white dots can be influenced by skin color, hair color, and excision tools used.3,4

Fig. 52B.10 Donor area hypopigmentation.
52B.4 Follicular Unit Excision Techniques
FUE is the removal of individual follicular clusters from the donor region using a punch. Follicular units historically have been defined as a pilosebaceous unit located at the mid-dermis of the scalp, situated approximately 1 mm apart. However, the term follicular unit is now commonly used to describe grafts without biopsy verification, both small grafts containing up to four hairs or, larger, more complex grafts, containing four or more hairs. This technique involves an incision and an extraction phase (Video 52B.1).
Follicular unit extraction FOX test: This is an older technique that allowed confirmation of a patient’s FUE candidacy based on excision of a few grafts from the donor region. The term was created by Drs. Bill Rassman and Bob Bernstein.9
Woods technique: This was the original term for FUE and was derived from Drs. Ray Woods and Angela Campbell.3,10 Here, harvesting of a single follicle from a group of follicles or portions of multiple follicular units might occur.
Follicular isolation technique (FIT): This was proposed by Dr. Paul Rose as a term to help accurately depict the procedure commonly called FUE.
Cole isolation technique (CIT): This term was developed by Dr. John Cole, and uses a depth control mechanism and a wide range of sharp punches.11 Low transection rates have been reported for CIT (<3%), even lower than those associated with the strip method. CIT can allow for such low transection rates as it varies the punch diameter, limits depth, and alters the tangential forces.
Harris surgically advanced follicular extraction (SAFE) technique12: Blunt punches ranging from 0.8 to 1.2 mm in size are attached to a rotating drill. There is full rotation of punches at different speeds and a fixed-depth stop can allow for a one-step dissection. The original manual technique was a two-step procedure, with a sharp punch scoring the surface of the skin, followed by use of a blunt punch.6,13
Robotic techniques: This incorporates the use of a robotic device or machine during the hair restoration process. Robotic techniques can help achieve high-quality FUE grafts and decrease the time required for harvesting. Automation can allow follicular unit density, hair angle, and punch insertion to be altered based on the information supplied by the physician. One example is the ARTAS robotic system.14
Body hair harvesting: Body hair is defined as hair from any region of the body excluding the scalp and can be a suitable alternative for individuals with depleted donor areas. Local anesthetic or topical lidocaine can be used to anesthetize the area prior to harvesting. A 0.8-mm sharp punch is a common choice; however, a modified hypodermic needle with a customized tip can be used to as well to harvest body hair. Yields can vary widely, ranging from 0 to 60%.15 Beard hair is located on the face, extends onto the neck, and grows faster than other body hair. While yields are variable, beard hair tends to have a higher yield than other body areas.
Beard hair harvesting: This is a form of body hair harvesting and is similar to scalp hair harvesting with differences occurring in graft distribution and recipient site creation. For beard reconstruction, a limit of 150 grafts is recommended if implanting harvested beard hair. For moustache reconstruction, it is best to use under the chin donor sites. A 0.8-mm sharp punch is a common choice for beard harvesting. Based on a meeting conducted by the British Association of Hair Restoration Surgery in July 2015, beards are used as a donor site in less than 5% of FUE cases.15
Suction-assisted excision: Negative pressure can be used to partially or fully remove a follicular unit during FUE.
52B.5 Graft Excision and Removal Related Terms
Rotational excision method: In this method, skin is penetrated using a punch that is rotated in repetitive 360-degree cycles usually with the assistance of a motor.
Oscillating excision: The punch is rotated through different arcs and repetitions per minute (RPMs) using a back and forth motion, either by hand or with a motor.
Rotating and oscillating excision method: This is when the penetrating punch is first rotated, and then oscillated. This method allows control of the rotational speed, rotation arc, rotation ramp, ramp of arc, and cycle duration.4,6
Vibrational excision: A vibratory transducer is used so that the punch vibrates as it penetrates the skin.
Axial force: This is the force that is applied parallel and down the centerline of the hair follicles. Axial forces can be evenly distributed (concentric) or unevenly distributed (eccentric). This force is usually greater on the inferior aspect of the tissue because the inferior margin of the punch touches the skin first. This is due to the angle of the hair growth and can create follicle displacement.
Tangential force: This is the force applied during rotation or oscillation.
Donor tension or traction: Traction can be applied to the donor area to help stabilize tissue fluidity. Tumescence, clamps, manual stretching, tensioner, or stapling can be used to apply desired tension.4,6
Scoring: This is the superficial cut that produces a circumferential or semicircle incision around the target follicular cluster, cutting through the epidermis and dermis layers of the skin.
Step method: Depending on which graft removal method is used, there are different steps involved. All graft removal methods share a final step: collection of the follicle using forceps or suction.
•One-step method: The excising punch is inserted to the desired depth and releases the follicle in one step. The single incision is created using a force generated through rotation, oscillation, axial action, or a combination of rotation and oscillation.
•Two-step method: This is similar to the one-step method as it also uses rotational, oscillation or axial action forces. Step 1 requires a sharp punch to score the skin using one of these forces. Step 2 requires a punch (same punch as step 1 or a second punch, dull or sharp) be inserted into the incision to the desired depth through rotation or oscillation.
•Three-step method: The two-step method is followed, with the skin scored using a sharp punch and then penetrated by another punch (sharp or dull). To complete this method and remove the graft, a sharp device (e.g., needle) is then used to cut the graft base while traction is applied using forceps.4,6
Dilek Erdogan Sequential (DES) technique: Developed by Dr. Koray Erdogan, in this method, the surgeon holds a punch in one hand and forceps in the other. Grafts are cut using the punch and then immediately removed using forceps, allowing harvesting to be performed in a rapid sequence.
Coring method: A sharp punch is inserted using a single axial force. This force is applied along the hair growth axis without rotation or oscillation. To loosen the graft, a tangential force can then be applied for removal using forceps.
Open (expanding needle) method (also called the Lift and Look method): In this method, a punch is used to score around the graft, followed by pulling the follicular cluster from the surface for observation. Once direction and splay are observed, correct maneuvers can be used to dissect the follicular unit. Suction can be of assistance to help clear the visual field.4,6
Sharp dissection: This uses a sharp punch to facilitate follicle excision.
Blunt dissection: A blunt (dull) punch can be used, which lacks a sharpened edge allowing for follicle separation from the surrounding tissues through a wedgelike configuration.
Pulling: Once the graft has been punched, an anterior traction can be used to help remove the graft.
Follicle distortion (reaction or physical movement of the follicles): This can occur due to the forces applied by FUE.4,6
Depth control: This can be created through using accessories that limit how deep the punch is inserted.
•Limited depth excision: This is limiting punch insertion to 1.8 to 3 mm to minimize follicle transection and allowing follicle extraction.
•Full depth excision: This is completely freeing the follicle by allowing the punch to be inserted 4 to 6 mm. At this depth, the punch can reach or exceed the bulbar region of the follicular group.
Bull’s eye: The follicles excised from a follicular group are centered in the punch during insertion.4,6
Delay in excision: This is the time difference between when the punch incises the graft and the time when the grafts are removed from the donor area.
Time out of body: This is the time between removing the graft from the donor area and inserting the graft into the recipient site. Grafts can be placed in a holding solution or immediately inserted into the recipient area.
Aid to extraction (ATOE, Cole Instruments; Fig. 52B.11): This instrument can hold up to 25 grafts at a time, encouraging rapid excision of punched grafts.4,6

Fig. 52B.11 Aid to extraction (ATOE).
Related posts:
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
 Transplanting into Areas of Cicatricial Alopecia
Transplanting into Areas of Cicatricial Alopecia
 Special Considerations for Postoperative Care in Follicular Unit Excision
Special Considerations for Postoperative Care in Follicular Unit Excision
 Hairline and Recipient Area Repair of Poor Previous Transplantation
Hairline and Recipient Area Repair of Poor Previous Transplantation
 Ergonomics in Hair Restoration Surgery: FUE Technique
Ergonomics in Hair Restoration Surgery: FUE Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


