Reconstruction of Mohs surgical defects is a challenging venture. A thorough understanding of skin physiology and anatomy (cosmetic subunits, relaxed skin tension lines, underlying neurovascular structures at risk, potential functional compromise, character of adjacent skin, and so forth), careful wound analysis, and meticulous operative techniques is key to a successful reconstruction. This article discusses in detail the use of local skin flaps and graft reconstruction.
Reconstruction of Mohs surgical defects is a challenging venture. A thorough understanding of skin physiology and anatomy (cosmetic subunits, relaxed skin tension lines, underlying neurovascular structures at risk, potential functional compromise, character of adjacent skin, and so forth), careful wound analysis, and meticulous operative techniques is key to a successful reconstruction.
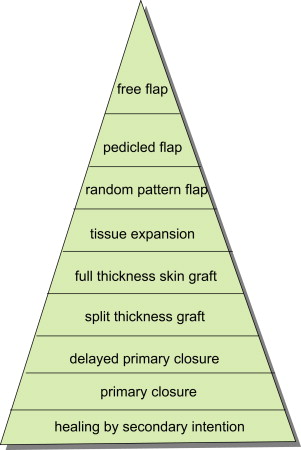
One of the cardinal principles in reconstructive surgery is function before form (ie, contour), and form before cosmesis. Preservation of the function is of utmost importance. Regardless of how beautiful a scar is, it is worthless if a patient’s ability to breathe or vision is impaired, for example. Change of contour (depressions or elevations) is more difficult to hide than a suboptimal scar. A reconstructive ladder is also often used in considering options for reconstruction with the order of from the least invasive to the most invasive. Healing by secondary intention is at the bottom of the ladder, followed by primary closure, graft, flap, and free flap ( Fig. 1 ). When there are multiple cosmetic subunits involved in a defect, combination closures with flap and/or graft and/or secondary intention should be considered to achieve an optimal reconstruction. This article discusses in detail the use of local skin flaps and graft reconstruction.
Preoperative planning
Preoperative consultation establishes an open communication between surgeon, patient, and family members. It provides a patient with a better understanding of the procedure by discussing the limitations and advantages of different reconstruction options. It also provides the opportunity for a surgeon to understand a patient’s aesthetic expectations and to evaluate a patient’s overall comorbidities, risk factors ( Box 1 ), and character and extent of the defect ( Box 2 ). In general, the simplest closure (healing by secondary intention or primary closure) is often the best option; it makes the fewest number of incisions and produces the least rearrangement of the tissue. Yet, when a defect is under high tension or with functional compromise, a flap is a good choice for redirecting tension lines, minimizing distortion of the tissue, and keeping the contours intact.
What are the patient’s age, occupation, and other daily activities?
Did the patient have previous radiation to the surgical site?
What is the patient’s aesthetic expectation?
Is the patient willing to go through and tolerate a multistaged repair?
Is the patient compliant in wound care? What is his/her living situation (family support system)?
What comorbidities may cause delayed wound healing (hypertension, heart disease, diabetes, organ transplant, immunosuppression, bleeding disorders, and smoking)?
Does the patient have a pacemaker/defibrillator?
Does the patient need prophylactic antibiotics?
Is the patient taking anticoagulants (aspirin, warfarin, clopidogrel, nonsteroidal anti-inflammatory drugs, vitamin E, fish oil, or herbal supplements)?
What type of cancer type does the patient have? Are the margins clear? What is the chance for recurrence?
What is the location and size of the defect?
What is the depth of the defect (partial thickness, full thickness, fat, fascia, muscle, cartilage, or bone; Any key structures exposed)?
What and how many cosmetic units and/or subunits are involved?
In which direction do the regional relaxed skin tension lines run?
How are the adjacent cosmetic boundaries associated with the defect?
Are free margins involved—nose, eyelids, and lips?
Is there compromise of function (ie, collapse of nasal valve, named nerve damage, and so forth)?
What are the quality, texture, laxity, and mobility of adjacent skin?
Flap reconstruction
A skin flap is defined as a construct of skin and subcutaneous tissue containing a direct vascular supply that is transferred to a primary surgical site adjacent to or near the flap.
Physiology of Skin Flaps
Adequate vascular supply to the flap and neovascularization between the flap and the recipient wound bed are critical factors to the survival of a flap. A wide interconnecting network of dermal and subdermal plexuses fed by septocutaneous and musculocutaneous arteries provides ample vascular supply to the skin.
Random pattern skin flaps and axial skin flaps are the primary flaps used in facial reconstruction. Random pattern skin flaps are supplied by musculocutaneous arteries close to the base of the flap that empty into the dermal plexus. Therefore, a good perfusion pressure from the supplying vascular network is important to prevent flap necrosis. Variable length-to-width ratios (2–4:1) have been suggested when designing random pattern skin flaps, depending on variable blood supplies at different wound defect locations. A wider skin flap, however, does not necessarily guarantee better survival.
The axial pattern flap (arterial flap) contains a specific named artery. Because of its dependable blood supply from the specific artery, it allows for the reconstruction of a more complex defect at a relative distant location, using the axial pattern flap. For example, the paramedian forehead flap, based on the supratrochlear artery, is often used in repairing large nasal defects. Axial pattern flaps are multistage flaps that are usually divided in 3 weeks after flap transfer once enough collateral vascular supply is established at the distal portion of the flap from the wound bed.
Flap Classification and Design
Flaps are classified in many ways based on:
- •
Location—local, regional, or distant
- •
Blood supply—random pattern or axial
- •
Configuration—bilobe or rhombic
- •
Method of transfer—pivotal, advancement, or hinge.
Flap design by method of transfer is the most common means of discussing the use of cutaneous facial flaps.
Advancement flaps
In advancement flaps, incisions are made so that the tissue is transferred by sliding toward the defect. They are usually constructed in a linear configuration. Unipedicle, bipedicle, and V-Y flaps are the principle types of advancement flaps.
- 1.
Unipedicle advancement flaps
In unipedicle advancement flaps, parallel incisions (often along the relaxed skin tension lines) are made to allow the flap and its pedicle to slide toward the defect. Undermining of the flap, around the pedicle and the defect, is important to reduce the tension and facilitates tissue movement. Because the length of advancement (defect width plus flap incision) is longer than the length of flap, it usually results in standing cone deformities. There are two main ways to eliminate the standing cones. Burow triangles can be excised along the longer sides to remove the standing cones. Alternatively, the rule of halves may be used when placing sutures to redistribute the extra length along the borders of the wound (defect plus the wound incision) evenly to eliminate the standing cones. Variations of unipedicle advancement flaps, such as U-plasty, H-plasty, and T-plasty (O to T or A to T), work particularly well in reconstructing certain locations: helical rim, chin, eyebrows, eyelids, medial cheek, and forehead ( Fig. 2 ).
- 2.
Bipedicle advancement flaps
Related posts:
 Mohs Micrographic Surgery Technique
Mohs Micrographic Surgery Technique
 Mohs Surgery for Squamous Cell Carcinoma
Mohs Surgery for Squamous Cell Carcinoma
 Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
 Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


