Flap Coverage of Thumb Defects
Kate Elzinga
Kevin C. Chung
DEFINITION
The thumb accounts for over 40% of hand function.1 Maintenance of length, ideally beyond the neck of the proximal phalanx, is critical for stable pinch and grasp.
The goals of thumb reconstruction include maximizing length, stability, strength, mobility, sensation, durability of coverage, and appearance while minimizing donor-site morbidity.
The function of the thumb is optimized following injury by restoring a sensate thumb pulp.2
ANATOMY
The volar thumb is covered by thick, durable, highly innervated, glabrous skin.
Dorsally, the nail provides protection for the distal phalanx and counterpressure for the pulp during pinch.
PATIENT HISTORY AND PHYSICAL FINDINGS
Following a thumb injury, important patient factors include age, sex, handedness, comorbidities, medications, allergies, occupation and avocations, and smoking status.
Injury factors to consider include the time and mechanism of injury, the degree of tissue contamination and necrosis, and any previous hand injuries.
The patients’ goals are explored. Their desire for a rapid return to work and their level of compliance and motivation are considered when formulating a reconstructive plan.
The thumb wound is examined, noting the level of the injury and tissue loss (skin, soft tissue, neurovascular bundles, tendons, bone, nail). Exposed structures are evaluated and documented.
The thumb’s color, capillary refill, turgor, and temperature are assessed as part of the vascular exam. The digital nerves are assessed using light touch, two-point discrimination, or the ten test.3
The function of the extensor pollicis longus and that of the flexor pollicis longus (FPL) are tested by asking the patient to actively flex and extend the interphalangeal (IP) joint of the thumb.
A digital block can be used for patient comfort to facilitate the examination following sensory testing of the thumb.
Donor sites are examined locally and regionally for thumb reconstruction.
IMAGING
Plain radiographs are performed for the thumb to assess for bony injury, level of amputation, and presence of a foreign body.
NONOPERATIVE MANAGEMENT
Small defects, up to 1 cm2 without exposed bone or tendon, heal well by secondary intention.
Ingrowth of glabrous skin results in durable, sensate coverage.
Moist, antibacterial dressings are applied daily.
Range-of-motion exercises are performed throughout to prevent stiffness.
Once healed, early use of the thumb is encouraged to help with desensitization of the fingertip and return of function.
Elevation of the injured upper extremity and gentle compression decrease edema at the thumb defect site, which expedites wound healing.
SURGICAL MANAGEMENT
Larger skin and subcutaneous tissue defects, over 1 cm2 without exposed tendon or bone, can be covered with a fullthickness skin graft (FTSG).
Rapid healing occurs, but FTSGs are less durable and have poorer sensory recovery compared with healing by secondary intention.
When tendon or bone is exposed, coverage with local and regional flaps is necessary.
To restore sensate, durable coverage over an exposed distal phalanx, flap reconstruction with a local Moberg flap can provide coverage for defects of 1.5 cm in length or up to 2.5 cm in length if a transverse proximal releasing incision is used (FIG 1).
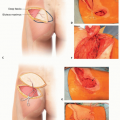
Larger defects can be covered with regional flaps such as the first dorsal metacarpal artery (FDMA) flap (FIG 2) or the reverse homodigital flap (FIG 3) based on the dorsal radial collateral artery.
The FDMA flap can be harvested up to 6 × 3 cm in size.
The reverse dorsoradial homodigital flap has been described from 2 × 2 cm up to 5 × 4 cm in size.4
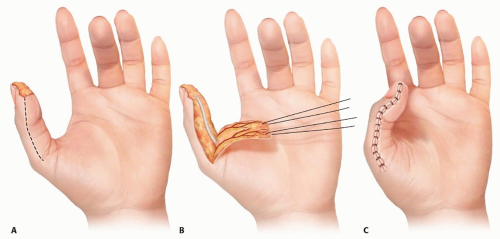 FIG 1 • The Moberg flap is designed over the volar thumb for coverage of distal thumb defects. A-C. Incisions are made at the midaxial line over the radial and ulnar digit up to the volar MCP joint crease. The radial and ulnar digital neurovascular bundles are elevated within the flap. The flap is elevated above the paratenon of the FPL and advanced distally. Flexion of the IP joint facilitates flap inset. |
Approach
The patient is positioned supine with the arm on a hand table.
Loupe magnification facilitates flap dissection.
The flap incisions are designed using a template of the defect prior to tourniquet inflation.
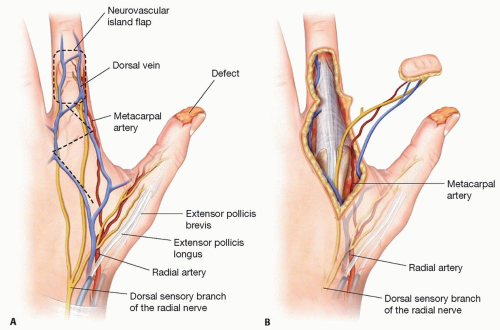
FIG 2 • The FDMA flap is elevated from the dorsal proximal phalanx of the index finger for coverage of thumb defects. A,B. The flap can be raised as an island flap, using a straight line, lazy S, or zigzag incision as shown here for elevation of the pedicle back to the flap pivot point, which is found just distal to the EPL tendon.
A tourniquet is used for flap elevation to create a bloodless field that facilitates exposure and decreases the risk of injury to the neurovascular structures supplying the flap.
Following flap elevation, the tourniquet is released. Flap perfusion is assessed. Hemostasis is achieved prior to flap inset to prevent a hematoma that could result in flap compromise.
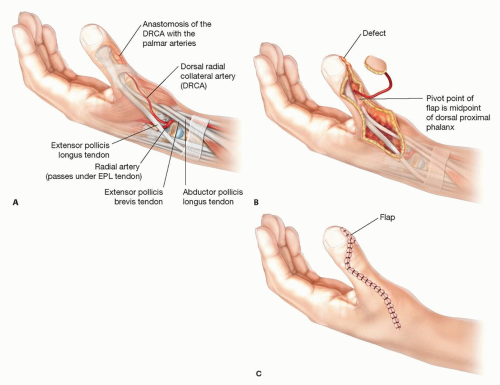 FIG 3 • A-C. The reverse dorsoradial homodigital flap is based on the anastomosis connection of the dorsal radial collateral artery and the palmar arteries of the thumb at the middle third of the thumb proximal phalanx. The flap is harvested as a distally based, reverse flap for coverage of distal thumb defects. |
TECHNIQUES
▪ Moberg Flap
Incisions are designed over the midaxial lines of the ulnar and radial thumb, at the junction of the glabrous and nonglabrous skin (TECH FIG 1A; see FIG 1). Proximally, the flap is marked to the metacarpophalangeal (MCP) joint crease bilaterally. If further advance is necessary, the flap can be extended proximal to the MCP, Burow triangles can be excised at the flap base bilaterally, or the flap can be advanced as a V-Y flap5 or as an island flap.6
The ulnar and radial digital nerves and arteries are elevated within the flap, which maintains the blood supply to the flap as well as innervation (TECH FIG 1B). The dorsal blood supply of the thumb from the princeps pollicis artery permits safe flap elevation without compromising the thumb’s perfusion.
When used as an island flap, a transverse, proximal releasing incision is made over the proximal phalanx (PP), connecting the two midaxial incisions. The radial and ulnar neurovascular bundles are protected. This release is seldom necessary because the thumb interphalangeal (IP) joint can be flexed sufficiently for the flap to cover the tip of the distal phalanx.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree