Flap Correction for Cryptotia
R. V. ARGAMASO
EDITORIAL COMMENT
This is an excellent flap for the correction of cryptotia, and all the editors recommend it to our readers. Correction of cryptotia is important not only from the standpoint of appearance, but it also allows the patient to wear glasses so that the helical portion of the rim frames does not slip off the ear.
A retroauricular retrograde skin flap can be used to correct a congenital, bilateral, ear deformity. The procedure places scar lines in areas that reduce scar visibility and also circumvents the need for skin grafts.
INDICATIONS
The term cryptotia is applied to a congenital anomaly of the ear characterized by the disappearance of the superior pole from view; the pole telescopes and hides beneath the scalp. When the invaginated upper pole is retracted out from under the scalp, the helix usually appears intact; however, the scapha may have some deformity associated with a rather sharply folded superior antihelical crus. A third crus may be present. After retraction is released, the upper pole returns into the scalp pocket.
Elevation of the upper pole of the ear from the side of the head is indicated for aesthetic reasons and also offers convenience and support for eye glasses or hearing aids. Many methods of releasing the upper pole have been described (1, 2, 3, 4, 5, 6). Elevation from the side of the head creates a skin
defect of the scalp and on the medial aspect of the ear. This open area requires coverage with adjacent scalp flaps, skin grafts, or a combination of these. The resultant scalp scars are readily seen but may be hidden if the hair is kept long.
defect of the scalp and on the medial aspect of the ear. This open area requires coverage with adjacent scalp flaps, skin grafts, or a combination of these. The resultant scalp scars are readily seen but may be hidden if the hair is kept long.
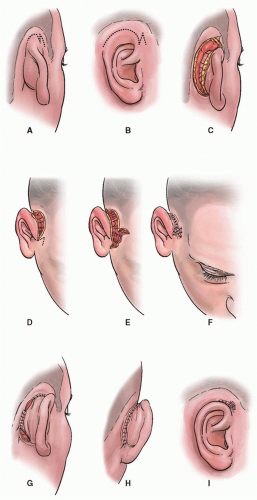 FIGURE 85.1 A-C: Artist’s rendition showing outline of skin incision on mastoid skin along the retroauricular sulcus, terminating anteriorly as a Z. Note back-cut toward the earlobe. D-F: Upper pole is released and triangular flaps are interposed. G-I: Retrograde flap is rotated and set in place.
Related posts: Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Inferior Turbinate Flap for Closure of Septal Perforations Inferior Turbinate Flap for Closure of Septal Perforations
 Postauricular and Retroauricular Scalping Flap (The Paras Flap) Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|