26. Fixation Devices
Brian H. Gander, Renato Saltz
BACKGROUND
■ Multiple devices have been described for fixation during browlift, midface lift, and neck rejuvenation.
• Plates and screws1: Screws can be removed during follow-up
• K-wires2: Can be either temporary or permanent
• Bolsters3
• Fibrin glue4
• Absorbable tack5
• Direct needle suture fixation
■ More recent methods of fixation use bioabsorbable devices that anchor soft tissues; however, permanent implantable devices are still in plastic surgeons’ armamentaria.
■ Barbed suture is a useful adjunct for rhytidectomy, body contouring, and breast surgery.
FIXATION FOR BROWLIFTS, MIDFACE LIFTS, AND NECKLIFTS
DIRECT NEEDLE SUTURE FIXATION
■ Uses permanent or absorbable suture depending on the surgeon’s preference
ENDOTINE TACK (COAPT SYSTEMS)6,7
■ Made of 82:18 ratio of polylactic acid/polyglycolic acid
■ Triangular tack 0.5 mm thick
■ Five tines up to 3.5 mm thick and a bone bolt 3.75 mm thick
■ To secure the tack, the Endotine drill bit is used to drill through the outer cortex of the calvarium. Octyl-2-cyanoacrylate (ISO-DENT, Ellman International) cement is used to fix device into the calvarium.
■ Soft tissues are secured to the tack using digital pressure.
■ Bioabsorbable
• Degrades through hydrolysis and enzymatic activity.
• The polyglycolic component goes through hydrolysis quicker than the polylactic acid component.
• The tack is completely absorbed in 12 months.
■ Advantages
• Speedy, direct fixation
• Bioabsorbs in 12 months
• Can be used in conjunction with an endoscope
• Low learning curve
■ Disadvantages
• Possibility of palpability until device absorbs
• Postoperative tenderness over the device
• Difficult to address temporal laxity and severe brow ptosis with the Endotine device
• Added cost to surgical procedure for the device
ULTRATINE TACK (COAPT SYSTEMS)8–10
■ The FDA approved the device in 2006.
■ Composed of polylactic acid and polyglycolic acid
• Ratio is unknown at this time given proprietary nature.
■ Undergoes hydrolysis at a faster rate than Endotine
• 50% of the device is absorbed in 4 months, and 70% is absorbed in 10 months.
■ Fixated to calvarium and soft tissues in same method as Endotine
■ Advantages
• Absorbs more rapidly than Endotine
• In one study with 12 patients who underwent coronal browlift, with one side fixated with Endotine and the other with Ultratine, decreased palpability and increased satisfaction noted on the Ultratine fixated side.10
■ Disadvantages
• Potential loss of fixation from quickened absorption
• Reports of inflammatory retention cysts that histologically demonstrated chronic granulomatous inflammation that has necessitated surgical correction8
• Added cost to the surgical procedure for the device
ENDOTINE RIBBON (COAPT SYSTEMS)11,12
■ Used for ptosis of cheeks, jowls, and neck
■ A 16 cm long ribbon 0.5 mm thick and 5 mm wide
■ Seventeen rows of double tines that are 2.5 mm tall, with holes between the tines. The proximal third of the device has no tines and is used as a “leash” and area for fixation.
■ Fixated to fascia with absorbable or permanent sutures
■ Same components and composition as Endotine tack
■ Bioabsorbable. This device loses its mass at 3 months and is absorbed in 12 months.
■ Advantages
• Useful adjunct for correction of ptosis at the cervicomental junction
• Can address temporal laxity12
• Same composition as Endotine tack and is absorbed in 12 months
■ Disadvantages
• Does not address anterior cervical banding
• Potential for palpability of the ribbon in patients with thin soft tissue
• Possible early loss of fixation when absorbable suture is used for fixation of the device
• Added cost to the surgical procedure for the device
MITEK ANCHOR (ETHICON)13
■ Can be used for medial and/or lateral canthoplasty
■ Allows fixation of soft tissues to bone
■ Three different sizes, with Mini-Mitek anchor most appropriate for facial aesthetic surgery
• The anchor portion is 1.8 mm in diameter, 5.4 mm in length. It is composed of a titanium alloy and has two barbs that are 180 degrees apart and angled retrograde for fixation against the cortical bone.
■ For fixation, a hole is drilled into the desired bone, and the anchor is inserted into the drilled hole.
■ Attached to the anchor is a double-armed suture of 3-0 Ethibond Excel (Ethicon) suture for fixation of soft tissues (braided polyester).
■ Advantage
• Ability to secure soft tissues to bone with relative ease
■ Disadvantages
• Potential for device to be palpable in area of thin soft tissue
• Permanent device
• Added cost to the surgical procedure
V-LOC BARBED SUTURE (COVIDIEN)14
■ Used in closure of skin and subcutaneous tissues in body contouring and breast surgery
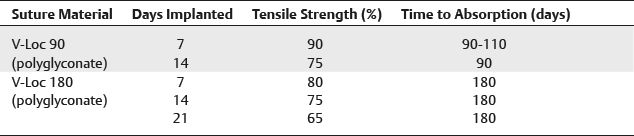
■ Composed of both bioabsorbable (polyglyconate) and permanent material of variable length (6, 12, 18, and 23 inches)
■ It is unidirectional barbed suture with a cutting or tapered needle at one end and a loop at other end for fixation.
■ The V-Loc suture is run in a subcutaneous or dermal plane in a single direction. To complete suturing, the V-Loc can be brought out through the skin at the edge of the wound, or, once the end of the wound has been reached, it can be run in the reverse direction for a number of passes and brought out through the skin.
■ Absorbable sutures have variable lengths of time for absorption (Table 26-1).
Table 26-1 V-Loc Suture Tensile Strength and Absorption Time