Fistulas, either between oral cavity and external face or between oral and nasal cavity, are major complications after microsurgical head and neck reconstruction. Any flaw in surgical planning, design, and execution may lead to this untoward outcome. Once fistula develops, it may interface with oncologic treatment, endanger the reconstruction, and increase overall patient suffering. This article analyzes individual factors involved in development of fistulas in spite of successful transfer of a free flap and proposes treatment guideline.
Key points
- •
Oronasal and orocutaneous fistulae are among the untoward results of reconstructive microsurgery in head and neck cancer in spite of free flap viability.
- •
Complete obliteration of ablation-related dead spaces, adequate volume replacement, and water-tight closure of oral wounds ensure uneventful healing and prevent fistulae.
- •
Management of fistula ideally should not delay radiotherapy. However, reconstruction is timed based on wound condition, with consideration not to interrupt oncologic treatment.
- •
A second free flap may become necessary for the treatment of fistulae.
Introduction
Orocutaneous or oronasal fistula following microsurgical head and neck reconstruction is a bothersome complication that downgrades patient’s quality of life and may jeopardize timely postoperative chemotherapy and radiotherapy administration.
In literature, the reported incidence of fistulae has been as high as 20%, and a large percentage of fistulas received major second operation to achieve wound healing. Reports dedicated to the causes of fistula, however, remain sparse and not comprehensive. Aside from the well-known patient-related risk factors such as poor nutritional status, systemic conditions that compromise wound healing, and radiotherapy and chemotherapy, knowledge on additional risk factors has been limited, in particular, the role of mistake in reconstructive surgery.
Furthermore, a systematic approach to head and neck fistulae after free flap reconstruction remains largely lacking. Wide-array of techniques such as vacuum-assisted closure, local and regional flaps, and free flaps in addition to medical treatment have been described but subjectively. The dilemma of deciding the optimal time for intervention with regards to adjuvant therapy administration and the optimal reconstructive option continues to confuse surgeons when confronted with a fistula.
Herein, this article will analyze fistulae from the perspective of poor planning, wrong design, and faulty execution of the surgery, and shares a simplified approach towards their management.
Introduction
Orocutaneous or oronasal fistula following microsurgical head and neck reconstruction is a bothersome complication that downgrades patient’s quality of life and may jeopardize timely postoperative chemotherapy and radiotherapy administration.
In literature, the reported incidence of fistulae has been as high as 20%, and a large percentage of fistulas received major second operation to achieve wound healing. Reports dedicated to the causes of fistula, however, remain sparse and not comprehensive. Aside from the well-known patient-related risk factors such as poor nutritional status, systemic conditions that compromise wound healing, and radiotherapy and chemotherapy, knowledge on additional risk factors has been limited, in particular, the role of mistake in reconstructive surgery.
Furthermore, a systematic approach to head and neck fistulae after free flap reconstruction remains largely lacking. Wide-array of techniques such as vacuum-assisted closure, local and regional flaps, and free flaps in addition to medical treatment have been described but subjectively. The dilemma of deciding the optimal time for intervention with regards to adjuvant therapy administration and the optimal reconstructive option continues to confuse surgeons when confronted with a fistula.
Herein, this article will analyze fistulae from the perspective of poor planning, wrong design, and faulty execution of the surgery, and shares a simplified approach towards their management.
Poor planning, in various defects
Poor planning can increase the risk of fistula, in particular, when the surgical plan results in improper flap selection to fulfill the reconstruction goal(s). The most common scenarios encountered include
Anterior mandibular defect with associated substantial glossectomy defect when a soft tissue flap and reconstruction plate is planned ( Fig. 1 )
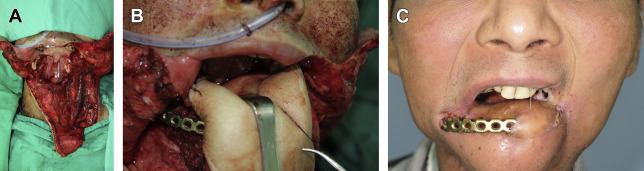
Fig. 1
( A ) The defect after resection involving the total tongue, total lower lip, right segmental mandibulectomy from left body to right angle, left marginal mandibulectomy, and left inferior maxillectomy. ( B ) In flap inset, the skin was brought on top of the plate, while the muscle was underneath it to obliterate dead space. ( C ) Plate exposure after radiotherapy.
A composite or extensive composite mandibular defect, LC or LCL type based on the Jewer and Boyd classification, when a soft tissue flap and reconstruction plate are chosen ( Fig. 2 )
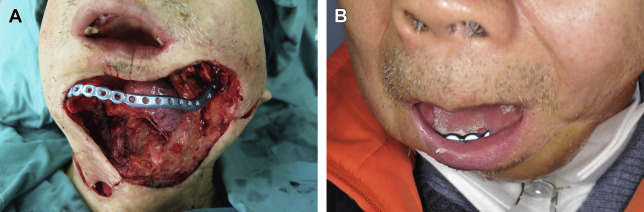
Fig. 2
( A ) Composite segmental mandibulectomy with partial glossectomy after tumor resection. ( B ) Plate exposure intraorally after radiotherapy.
A high-volume maxillary defect when a bone flap is used
Ideally, the first 2 scenarios should be reconstructed with double free flaps, a vascularized bone flap for segmental bone defect and soft tissue flap for dead space obliteration, soft tissue replacement, or coverage reconstruction ( Fig. 3 ). This option is associated with significantly fewer complications compared with the soft tissue flap and reconstruction plate option. On the other hand, the third scenario is better reconstructed with soft tissue flap to obliterate the dead space followed by bony reconstruction in a second stage.
Defective planning leading to fistula can also include failure to identify and obliterate potential dead spaces after ablation surgeries. Such dead spaces may necessitate additional tissue components, larger skin paddle, particular inset techniques, or even a second free flap. Neglecting those inapt designs or faulty executions of reconstruction may lead to fistulae complication.
In the commonly encountered glossectomy and mouth floor defects, the dead space following the resection of extrinsic tongue muscles needs to be obliterated adequately, not only to prevent fistulization, but also to support the neotongue for better function. It is worth noting that a deliberate suboptimal reconstructive plan is necessary sometime. As stated in another article (see Nidal Farhan AL Deek, Fu-Chan Wei, and Huang-Kai Kao’s article, “ Free Tissue Transfer to Head and Neck: Lessons Learned from the Unfavorable Results—Experience per Subsite ,” in this issue), the surgeon may need to compromise by adopting a staged reconstruction with a free flap for the purpose of wound coverage only. This staged approach is deliberately chosen with complete awareness of possible tradeoffs such as fistula and other complications due to poor prognosis of the case. The situation is usually encountered in massive composite defects after ablation of recurrent or advanced secondary and tertiary tumors that otherwise should be reconstructed by double free flaps. The decision making, therefore, should always be guided by sound risk–benefit approach.
Inapt design
Given that the proper flaps have been chosen, design remains essential to fulfill the reconstructive goals. Dead space obliteration is 1 of these key goals; when not adequately fulfilled it may become a major risk factor for complications, including fistula. The flap, therefore, should be properly designed, ideally by an experienced surgeon to bring a reliable, suitably sized muscle or dermoadipofascial part of the skin paddle to achieve the goal. The dead space between the hyoid bone and the mandible originally occupied by extrinsic tongue muscles can be a good example to illustrate the importance of good flap design. This space is usually about 5 × 3 × 3 cm in volume, and a reliable muscle segment can be included to fill the defect without compromising the viability of the rest of the flap and tongue reconstruction. A composite design of the myocutaneous flap, even made bigger than needed, may not be able to reconstruct the tongue and obliterate the dead space at the same time, while a combined flap design could be more reliable in achieving this goal ( Fig. 4 ).
Related posts:
 The Unfavorable Outcome: Here We Conquer
The Triangle of Unfavorable Outcomes After Microsurgical Head and Neck Reconstruction
Mayo Clinic Experience with Unfavorable Results After Free Tissue Transfer to Head and Neck
Unfavorable Results After Free Tissue Transfer to Head and Neck
Henri Mondor Experience with Microsurgical Head and Neck Reconstruction Failure
The Osteosarcoradionecrosis as an Unfavorable Result Following Head and Neck Tumor Ablation and Microsurgical Reconstruction
The Unfavorable Outcome: Here We Conquer
The Triangle of Unfavorable Outcomes After Microsurgical Head and Neck Reconstruction
Mayo Clinic Experience with Unfavorable Results After Free Tissue Transfer to Head and Neck
Unfavorable Results After Free Tissue Transfer to Head and Neck
Henri Mondor Experience with Microsurgical Head and Neck Reconstruction Failure
The Osteosarcoradionecrosis as an Unfavorable Result Following Head and Neck Tumor Ablation and Microsurgical Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


