Female genital mutilation (FGM) has become more common in the United States with increased immigration to the United States of individuals from areas where the practice is endemic. Although the root causes of FGM may be multiple, the practice is banned in the United States on all women under age 18 and is increasingly being outlawed by individual state legislatures. American dermatologists should expect to see a growing number of patients having undergone FGM who may present with complications ranging from keloids and epidermal cysts to clitoral neuromas and abscess formation. While treatment of such complications is often elusive and unsuccessful, recognition of the practice may prevent future patient abuse and death. The eradication of FGM will require the concerted efforts of many individuals, both within and outside of the health care field, with dermatologists poised to play a crucial role in diagnosis and management in the near future.
Female genital mutilation (FGM) is a condition with which dermatologists should be familiarized, as it likely will be seen with rising frequency in the American dermatologist’s clinic. With increased immigration of individuals from regions where the practice is endemic to the United States and other industrialized nations, FGM has gained growing attention. FGM was formally defined by the World Health Organization (WHO), United Nations Population Fund (UNFPA), and the United Nations Children’s Fund (UNICEF) as that which
“comprises all procedures involving partial or total removal of the external female genitalia or other injury to the female genital organs whether for cultural or other non-therapeutic reasons ”
Estimates of the prevalence of the practice vary on a regional basis, with WHO estimating in 1998 that 137 million women underwent the procedure, and a further two million girls are at risk each year. In the United States, an estimated 168,000 women in 1990 were believed to either have undergone or to be at risk of FGM ( Fig. 1 ).

While the practice of altering a woman or girl’s genitalia has been alternatively termed circumcision or ritual female genital surgery among other names, the term mutilation may best convey the sheer impact of the procedure on both a psychological and physical sense. FGM is known to be associated with innumerable changes in a female’s life, from decreased fertility to increased risk of dermatologic complications to potentially elevated risk of human immunodeficiency virus (HIV) contraction. Dermatologists seeking to reduce the incidence of FGM must be cognizant of the risks to victims arising from the practice, but also understand that FGM is a form of child and female abuse that is both medically dangerous and socially unacceptable in that it ultimately victimizes women.
This article aims to (1) explain the widely used WHO classification system for FGM, (2) discuss the prevalence of FGM in the United States, (3) provide a review on dermatologic complications of the procedure, and (4) offer suggestions to dermatologists working with women who have been victims of FGM.
Classification
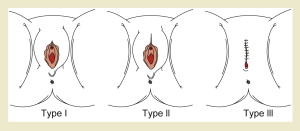
Currently, the WHO, UNFPA, and UNICEF have classified FGM into four types ( Fig. 2 ) :
Type 1. Clitoridectomy: partial or total removal of the clitoris, with or without removal of the prepuce.
Type 2. Excision: partial or total removal of the clitoris and labia minora, with or without excision of the labia majora.
Type 3. Infibulation: narrowing of the vaginal opening through creation of a covering seal. The seal is formed by cutting and then moving the inner (and sometimes the outer) labia. Infibulation may be performed with or without clitoral excision. This practice is the most severe form of FGM. Women must have their legs bound for a period of 1 to 4 weeks following the procedure to allow for healing of tissues and fusion of the labia majora. Deinfibulation, or the widening of the vaginal opening (typically before childbirth), is either performed by the husband during intercourse or by a physician or FGM practitioner. Following childbirth, a woman may have a reinfibulation procedure, whereby her vaginal opening is once again narrowed.
Type 4. All other harmful procedures to the female genitalia for any nontherapeutic purpose, including pricking, piercing, incising, scraping, and cauterizing of the genital area.
Related posts:
 Buruli Ulcer: Advances in Understanding Mycobacterium ulceransInfection
Buruli Ulcer: Advances in Understanding Mycobacterium ulceransInfection
 Outbreak of Nontuberculous Mycobacterial Disease in the Central Pacific
Outbreak of Nontuberculous Mycobacterial Disease in the Central Pacific
 Arsenical Keratoses in Bangladesh—Update and Prevention Strategies
Arsenical Keratoses in Bangladesh—Update and Prevention Strategies
 Chagas Disease: Coming to a Place Near You
Chagas Disease: Coming to a Place Near You
 Widespread Use of Toxic Skin Lightening Compounds: Medical and Psychosocial Aspects
Human Immunodeficiency Virus and Leprosy: An Update
Widespread Use of Toxic Skin Lightening Compounds: Medical and Psychosocial Aspects
Human Immunodeficiency Virus and Leprosy: An Update
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


