and Peter M. Prendergast2
(1)
Elysium Aesthetics, Bogota, Colombia
(2)
Venus Medical, Dublin, Ireland
Introduction
There is a rising demand for aesthetic enhancement of the breast (Fig. 16.1). The use of implants is still considered the gold standard to improve the volume and shape of the female breast. However, many patients who desire augmentation still have reservations and concerns about the use of silicone or saline implants. Autologous fat provides an alternative to implants for moderate augmentation and contouring of the breast [1].
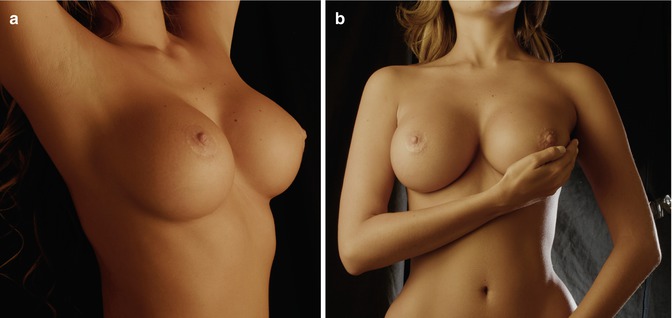
Fig. 16.1
Aesthetically ideal female breasts (a, b)
Fat was first proposed as a filling material by Neuber in 1893. The concept rapidly gained momentum, and subsequent work by Guerrero Santos, Bircoll, Coleman [2], and others has shown that it is possible and safe to harvest and graft fat for rejuvenation of the face and contouring of the body, provided it is handled with care [1, 3].
Fat has many attributes of the ideal filler. It is natural, soft, and safe and has the potential for permanence if it acquires a new blood supply following placement in the recipient site. Since breast fat grafting is technique dependent, the long-term results are variable [4–6]. We use VASER ultrasound to emulsify fat before extraction, a process that does not compromise viability of the adipocytes.
The breast has a rounded shape defined by the breast gland contour. The anatomical features surrounding the breast gland enhance its shape and projection. The triangular area between the clavicle and the anterior insertion of the deltoid muscle; the axillary portion of the gland, or Spence’s tail; and the negative space lateral to the gland, should follow a lazy “S.”
Stealth Incisions
The ideal incisions should be made with the patient in the supine position, with a 90° arm abduction. Five-millimeter incisions are placed in the anterior axillary fold, in the areola, and in the inframammary fold.
The ports are placed in the incisions and sutured in place (Fig. 16.2).

Fig. 16.2
Incisions with ports at the anterior axillary fold and in the inframammary fold
The Use of Drains
Drains are not necessary in the breast. The fat injections are performed by accessing the breast tissue through the anterior axillary fold incisions. These incisions should be closed to avoid leakage of fat following the procedure.
Marking
Deep Markings
With the patient in the standing position, outline the gland. Mark the areas that need more projection. This is usually the upper poles of the breast. Most of the fat will be injected in these areas. Mark the surrounding area of the breast, from the axilla lateral to Spence’s tail to the lower portion of the lateral chest wall (Fig. 16.3). These surrounding areas will be treated with thorough fat removal in order to enhance the relative size and shape of the breast itself.
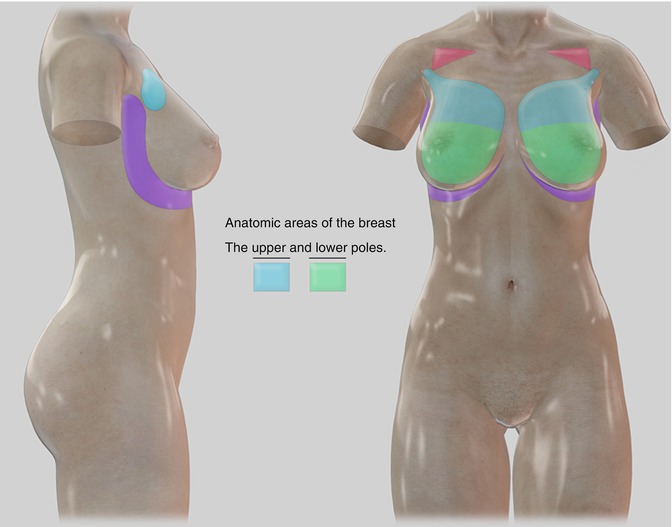
Fig. 16.3
Anatomical areas of the breast, upper and lower poles (green and blue), the subclavicular triangle (red), the peripheral area around teh breast (purple). On the lateral view, note the tail of Spence extending towards the axilla
Framing
Little framing is needed in the breast area. However, a slight delineation of the pectoralis border at the upper limit of the breast enhances the breast shape and increases muscular definition. The lateral “S” is marked to define the smooth contours of the breast.
Negative Space
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


