and Peter M. Prendergast2
(1)
Elysium Aesthetics, Bogota, Colombia
(2)
Venus Medical, Dublin, Ireland
Introduction
One of the most appealing characteristics of an athletic male body is a well-defined pectoral area (Fig. 9.1). The aesthetic standards for the male chest are strongly correlated with the shape and development of the pectoralis muscles. Abnormal fat deposition in the chest, gynecomastia, trauma, and congenital abnormalities distort the normal anatomy and are a common motivation to perform reshaping surgery. In addition, underdevelopment of the male chest musculature seems to be a result of modern urban lifestyle choices, including increased calorie intake, lack of physical activity, and resistance exercises. Most of the treatment options are focused on correcting the chest deficiencies and deformities

[1–3].
Fig. 9.1
Athletic male chest: notice the muscular shape of the pectoralis muscle in the superficial
The ideal male chest is defined by the exposure of the surface anatomy, which is a reflection of the disposition and development of the pectoralis muscles. Although it is a reflection of the muscle mass itself, the surrounding areas must also be treated in order to produce optimal definition [4, 5].
The anatomy of the pectoral area is divided into specific zones to fulfill the goals of the technique (Fig. 9.2).

Fig. 9.2
Upper: light green, and lower pole: dark green
For years, implants have been considered the gold-standard method for treating pectoral deficiencies [2]. However, their shortcomings include expensive prostheses and potentially serious complications, including a poor aesthetic result and a “female”-like appearance. With fat grafting and superficial liposuction, we can produce superior results compared to these traditional methods, thus making it a good alternative for male chest reconstruction [6, 7]. For the purposes of fat grafting and planning, the pectoralis major is divided into upper and lower poles. Aesthetically, the upper pole should have a greater volume than the lower pole, due to the greater muscle mass, so most of the fat will be grafted to this region.
The anatomical features surrounding the pectoralis muscle are divided into five “negative spaces”: areas that should be concave in order to enhance the convexity of the pectoralis and surrounding muscles (Fig. 9.3).
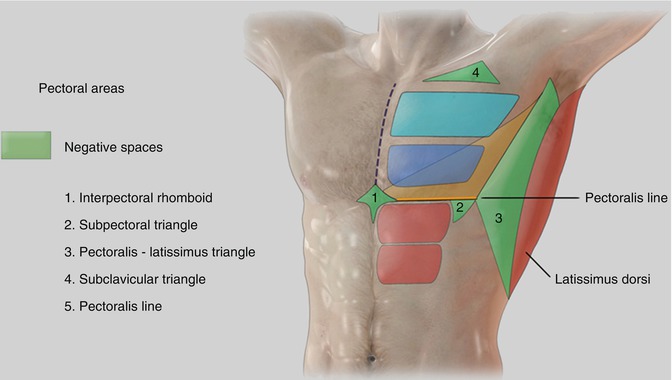
Fig. 9.3
Negative areas surrounding the pectoralis muscle (in green), upper pectoralis pole (in light blue), and lower pole (in dark blue)
The first negative space is a rhomboid between the inferior borders of the pectoralis major, the xiphoid process, and the origin of the rectus abdominis at the midline (interpectoral rhomboid).
The second area is a triangle defined by the pectoral line and the lateral border of the rectus abdominis (subpectoral triangle). This area must be treated aggressively with subdermal and intermediate liposuction. It also links the definition of the pectoralis muscles with definition of the abdomen.
The third area is the triangular area between the lateral border of the pectoralis major and the lateral border of the latissimus dorsi (pectoralis–latissimus triangle). Even though this is beyond the pectoral area, in the contouring process it is important to expand the concavity to this limit.
The fourth area is defined as the triangular area bordered by the clavicle, deltoid, and clavicular portion of the pectoralis major (subclavicular or deltopectoral triangle).
The fifth area is a horizontal line along the inferior border of the pectoralis major, usually 1 cm below the nipple level (pectoralis line). This represents a negative space that softens along the lateral border of the muscle toward the upper pole.
Finally, a triangular area defined by three points: the inferolateral corner of the pectoralis major, the medial point of the pectoral line, and the lateral insertion of the pectoralis major. This area is essentially the lower lateral pole of the pectoral area. Deep liposuction should be performed in this area in obese and gynecomastic patients, sometimes extending to the limits of the fatty tissue beyond the underlying pectoral muscle [5].
Stealth Incisions
Ideally, the incisions should be placed with the patient in the supine position, with the arms abducted to 90°. Two 5 mm incisions are placed bilaterally, in the anterior axillary fold and in the areola just below the nipple. Silicone ports are placed into the incisions and sutured in place (Fig. 9.4).

Fig. 9.4
Anterior axillary and sub-nipple incisions with ports stitched in place
The Use of Drains
The use of drains is not necessary in this area. In fact, the anterior axillary incisions are the preferred access sites for fat grafting. As such, it is mandatory to close these incisions to avoid retrograde fat leakage through the incision points.
Markings
Deep Markings
In the standing position, first mark the fat deposits to be removed with deep liposuction. Usually, there is extra fat around the nipples that extends beyond the border of the pectoralis muscles. Mark this area. For a clear upper limit, a triangular area between the inferomedial border of the pectoralis major and the anterior axillary fold is marked (Fig. 9.5).
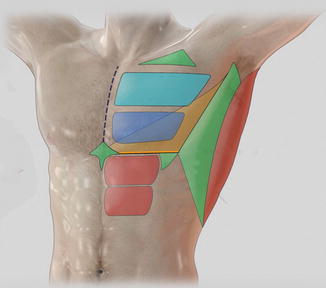
Fig. 9.5
Pectoral zones, negative spaces (in green). Deep extraction is shown as the triangular yellow zone, above it deep extraction should not be performed
Mark the depressions or areas that need more projection in the pectoralis, especially the upper pole. These areas will be treated with fat grafting.
Framing
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


