Sam Lam, Thomas Tzikas, and Mark Glasgold address questions for discussion and debate:
- 1.
With the increase in alloplastic injectables, is fat grafting dead?
- 2.
Where do you think fat grafting fits in compared with the injectable implants?
- 3.
Do you do grafting and injectables in some patients? If so, give examples.
- 4.
How do you harvest and prepare fat for injection? Do you think that the process chosen impacts longevity of the grafts, and how long does fat last in your experience? What percentage usually takes in each site, and does the source or the site injected make a difference in this regard?
- 5.
What areas of the face are most amenable to fat grafting, and how much fat should ideally be injected into each site?
- 6.
Analysis: Over the past 5 years, how has your perspective evolved or what is the most important thing you have learned/observed regarding fat grafting?
Samuel Lam, Thomas L. Tzikas, and Mark Glasgold address questions for discussion and debate:
- 1.
With the increase in alloplastic injectables, is fat grafting dead?
- 2.
Where do you think fat grafting fits in compared with the injectable implants?
- 3.
Do you do grafting and injectables in some patients? If so, give examples .
- 4.
- 5.
- 6.
With the increase in alloplastic injectables, is fat grafting dead?
Lam
The answer is absolutely not. Fat grafting and fillers are both viable methods for facial rejuvenation and enhancement. Injectable fillers provide immediate gratification and minimal downtime for patients who are interested in using them. However, for someone with more substantive aging that requires multiple syringes, fat can provide more global restoration and be more durable than injectable fillers, which is discussed in the subsequent questions.
Tzikas
On the contrary, fat grafting is more popular today and is performed by more physicians than at any other time. Injectable fillers have actually reinforced the idea that facial volume is the main consideration when attempting to restore youthful qualities to the aging face. Although injectable fillers are fairly straightforward and simple to perform, they alone cannot give the overall pan-facial improvement that fat grafting can. In my practice, facial fillers play an important role in introducing new patients to facial rejuvenation. Patients see an improvement in their facial appearance but, over the course of repeated injections and over a few years, many patients develop injection fatigue and desire a longer-lasting and more significant result. Fat grafting is the perfect logical next step in their rejuvenation and is almost always accompanied by other procedures, such as eyelid rejuvenation, laser skin treatment, or facelift surgery. Fat grafting provides a soft tissue layer of padding that aging patients are missing while improving the overall appearance and quality of the skin.
Injectable fillers are limited by volume and cost. It would be cost prohibitive to inject 10 or 20 syringes of a hyaluronic acid filler or calcium hydroxylapatite in a patient but this can easily be done with fat. The important distinction, however, is that fat is not an ideal filler for facial lines, such as nasolabial folds or glabellar creases. The method of injection is also different. Fat is injected in the deeper tissue planes and, therefore, requires a greater volume to augment an area.
There will most likely always be a place for alloplastic facial fillers because of their unique qualities, such as the superficial filling of facial lines. It is not that fat cannot fill these lines as well as the fillers, it can. Fat is presented to patients as a longer-lasting augmentation product and in areas, such as superficial facial folds in mobile regions, it is not better than the fillers with respect to longevity. Fat grafting, however, does give some long-term augmentation even in these areas but the percentage of fat taking is much less than in the less-superficial and less-mobile facial areas.
Where do you think fat grafting fits in compared with the injectable implants?
Lam
Alloplastic injectables can be a wonderful alternative to fat grafting, but each modality carries it owns merits, risks, and limitations. Fat grafting is a live graft that carries the risk of changes with weight gain or loss along with other metabolic changes that can occur with aging. Those who fluctuate in weight or are of prechildbearing age are on the higher-risk profile when working with fat grafting. In those patients, I prefer injectable fillers for their safety. In addition, younger patients or those who are overweight typically need fewer syringes of injectable product making it more cost beneficial to use off-the-shelf fillers. However, in someone aged more than 40 years, for example, who has ongoing hollowness of the face, I often need 40 to 50 mL of fat to achieve a remarkable global rejuvenation. I think each syringe of filler is equal to about 3 syringes of fat. Accordingly, it can become cost prohibitive to provide that degree of injectable product for a patient’s face when harvested fat is free, so to speak. I also find that fat grafting provides a much softer look and feel to the face that may be partially attributable to stem cell effects (but I am not convinced entirely of this observation) but also because fat is softer in texture.
The limitation of fat grafting is that because it is a live graft it does not have 100% take, meaning that it is less predictable in any one area of the face than fillers would be. Therefore, if someone is interested in just having their cheeks augmented, it makes less sense for me to undertake a surgical procedure just to put some fat in the cheeks. I think it is more predictable to use fillers in this case. Also, with a permanent filler, like fat grafting, I think a person looks better when the permanent filler is blended evenly over multiple small areas rather than just stuck in one area of the face. Further, because fat is a very soft product it may not lift folds or creases or small skin divots as effectively as soft tissue fillers. I oftentimes use soft tissue fillers to augment my fat-grafting results when I see small areas that could use just a little bit more fat but where I think a fat graft would be unpredictable if the person went back under anesthesia and had a little more fat put in. I use the analogy of a bed to understand how I conceptualize the face for prospective patients. I think fat provides the mattress to the face; whereas fillers are the duvet that can fill in more surface problems. Neurotoxins and skin care can help with the outer sheets of the bed. In this way, I try to communicate with patients the benefits and limitations of fillers and fat grafting.
Tzikas
In the first discussion I respond, in part, to this question. Additionally, one facial filler that has some of the attributes of fat grafting is poly-L-lactic acid. With repeated treatments, it results in a softness to facial areas, such as the midface, that resembles the appearance one can obtain with fat grafting. Poly-L-lactic acid has several limitations, however, most notably related to areas that it should not be injected because of the high incidence of nodules, which are not easily treated. Two such areas are the infraorbital region ( Fig. 1 A, B) and the lips. Fat grafting can be used in these areas with excellent outcomes, although more limited in the lips, and with an extremely low risk of complications.
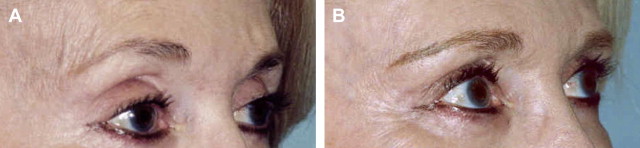
Fat grafting should be thought of as a pan-facial augmentation product because the face undergoes volume loss. Obviously, it is a more complex procedure than the injection of facial fillers and requires more training by the surgeon and with more recovery time for patients. Fat grafting requires that adequate volumes be injected to the face (at least 50 mL for the face) in a multilayered technique. My observations have been that the results seem to be softer over several years ( Fig. 2 A, B).

Where do you think fat grafting fits in compared with the injectable implants?
Lam
Alloplastic injectables can be a wonderful alternative to fat grafting, but each modality carries it owns merits, risks, and limitations. Fat grafting is a live graft that carries the risk of changes with weight gain or loss along with other metabolic changes that can occur with aging. Those who fluctuate in weight or are of prechildbearing age are on the higher-risk profile when working with fat grafting. In those patients, I prefer injectable fillers for their safety. In addition, younger patients or those who are overweight typically need fewer syringes of injectable product making it more cost beneficial to use off-the-shelf fillers. However, in someone aged more than 40 years, for example, who has ongoing hollowness of the face, I often need 40 to 50 mL of fat to achieve a remarkable global rejuvenation. I think each syringe of filler is equal to about 3 syringes of fat. Accordingly, it can become cost prohibitive to provide that degree of injectable product for a patient’s face when harvested fat is free, so to speak. I also find that fat grafting provides a much softer look and feel to the face that may be partially attributable to stem cell effects (but I am not convinced entirely of this observation) but also because fat is softer in texture.
The limitation of fat grafting is that because it is a live graft it does not have 100% take, meaning that it is less predictable in any one area of the face than fillers would be. Therefore, if someone is interested in just having their cheeks augmented, it makes less sense for me to undertake a surgical procedure just to put some fat in the cheeks. I think it is more predictable to use fillers in this case. Also, with a permanent filler, like fat grafting, I think a person looks better when the permanent filler is blended evenly over multiple small areas rather than just stuck in one area of the face. Further, because fat is a very soft product it may not lift folds or creases or small skin divots as effectively as soft tissue fillers. I oftentimes use soft tissue fillers to augment my fat-grafting results when I see small areas that could use just a little bit more fat but where I think a fat graft would be unpredictable if the person went back under anesthesia and had a little more fat put in. I use the analogy of a bed to understand how I conceptualize the face for prospective patients. I think fat provides the mattress to the face; whereas fillers are the duvet that can fill in more surface problems. Neurotoxins and skin care can help with the outer sheets of the bed. In this way, I try to communicate with patients the benefits and limitations of fillers and fat grafting.
Tzikas
In the first discussion I respond, in part, to this question. Additionally, one facial filler that has some of the attributes of fat grafting is poly-L-lactic acid. With repeated treatments, it results in a softness to facial areas, such as the midface, that resembles the appearance one can obtain with fat grafting. Poly-L-lactic acid has several limitations, however, most notably related to areas that it should not be injected because of the high incidence of nodules, which are not easily treated. Two such areas are the infraorbital region ( Fig. 1 A, B) and the lips. Fat grafting can be used in these areas with excellent outcomes, although more limited in the lips, and with an extremely low risk of complications.
Fat grafting should be thought of as a pan-facial augmentation product because the face undergoes volume loss. Obviously, it is a more complex procedure than the injection of facial fillers and requires more training by the surgeon and with more recovery time for patients. Fat grafting requires that adequate volumes be injected to the face (at least 50 mL for the face) in a multilayered technique. My observations have been that the results seem to be softer over several years ( Fig. 2 A, B).
Do you do grafting and injectables in some patients? If so, give examples
Lam
Yes, as elaborated in question 2 ( Where do you think fat grafting fits in compared with the injectable implants? ), I use fat grafting for specific patients and fillers for others and in some cases I use both. Let me clarify by being more succinct. I prefer fillers for those who are metabolically unstable to have safe fat grafting (too young or with fluctuating weight profiles); those who want just a little area of the face managed, like the cheek, lips, or nasolabial grooves; those who have limited downtime or must be looking good for an upcoming event that is soon; those who are afraid of fat grafting or do not understand it; those who cannot afford to have fat grafting but just want a little injectable filler (I like to say that is like buying a little bit of fat grafting at a time); those who simply do not have enough donor fat to do sufficient work; those who have had fat grafting and would like a touch up or to maintain their result against further aging; and those who are unsafe surgical candidates for whatever reason.
For me, fat grafting is suggested for those individuals who want the best global, durable, and beautiful results and can afford to undergo the procedure in terms of cost, recovery, and safety (as described previously). I like to look at fat grafting as the Ferrari of results because I really do not think facial fillers can get close to the beauty and softness of a fat-grafting result when it is done well and artistically by an experienced practitioner of this art and science.
Tzikas
Yes, fat grafting is often used for augmenting the face as a standalone procedure or it can be used to augment the midface and upper face when combined with several types of surgeries, such as fractional CO 2 laser resurfacing, blepharoplasty, facelift, or even rhinoplasty. On many occasions, the fine perioral lines are treated with microdroplet Silikon-1000 (Alcon Labs, Fort Worth, TX, USA) injections at the same time. This treatment is an off-label Food and Drug Administration (FDA) use of this product but has been rewarding for this application in my practice. Other fillers, such as hyaluronic acids or calcium hydroxylapatite, are sometimes used in conjunction with fat to fill in the superficial portion of a nasolabial or glabellar fold for which fat does not correct as well.
A cost-effective procedure that has become popular in my older patient population is a combination of moderate volume (20–30 mL) midfacial and upper-facial fat grafting with a silicone injection to the perioral rhytids and fractional CO 2 laser resurfacing of the face. This procedure provides correction of the 2 major components of facial aging, volume loss in the midface and facial rhytids caused by environmental factors, with a short recovery time of 7 to 10 days.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


