13 Eyebrow height / shaping
Summary and Key Features
• Eyebrow height and shape play a key role in attractiveness, emotional expression, and perceived youthfulness; the ideal brow for an individual depends on many factors
• Enhancement of brow height and contour following treatment with botulinum toxin is well documented
• The standard injection pattern in the glabella leads to inactivation of the brow depressors and portions of the frontalis; it is likely that the compensatory increase in the resting tone of the frontalis leads to brow elevation
• Brow ptosis and a ‘mephisto’ brow are the most common complications of treatment and an understanding of the relevant anatomy can help to prevent this
• Hyaluronic acid fillers can be a useful adjunct to botulinum toxin if there has been volume loss beneath the brows
• Eyebrow asymmetry is a common problem and symmetric treatment with botulinum toxin may offer a simple, non-surgical, method of correction
Eyebrows and attractiveness
The modern concept of the ideal contour of the female brow was proposed by Westmore in 1974 (Fig. 13.1). This schema applies best to an oval-shaped face, and serves as a good starting point since there is no clear definition of an ‘ideal brow’ that can be applied to all faces (Fig. 13.2). Several authors have suggested that the ideal apex of the brow is actually more lateral than the lateral limbus as Westmore had proposed. If the apex is too medial and overelevated it creates a surprised appearance.
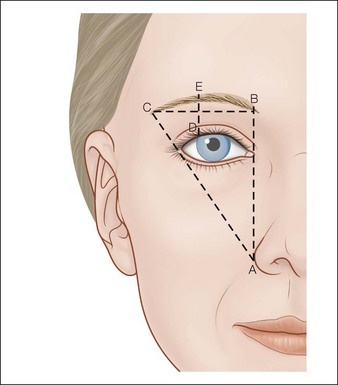
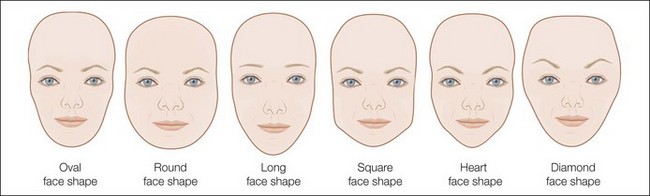
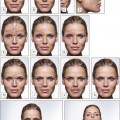
Figure 13.2 Face shapes.
Round face – to make the face appear more oval eyebrow lines should go up. A high arched brow with a lateral apex is ideal.
Long face – horizontal eyebrows draw the eye from side to side, making the face appear more oval.
Square face – angled brows balance the strong jaw line. The apex of the brow should be above the square of the jaw if possible.
Heart-shaped face – a rounded brow adds curves, softens the appearance, and emphasizes the shape.
Diamond face – a rounded brow will soften the angular face. If the face is particularly wide a peaked brow will draw the eyes up and make the face appear more oval.
Variations to Westmore’s ideal brow have been suggested to account for variations in face shape and intercanthal distance. Baker et al confirmed that, in the case of a long face and square face, observers preferred eyebrows planned by a makeup artist who accounted for these factors, rather than the Westmore ideal (see Fig. 13.2, Box 13.1).