(1)
Division of Plastic-, Hand-, and Microsurgery Department of Surgery, Ludwig Maximilians University, Munich, Germany
2.1 Experiments and Training in Rats
Also experienced microsurgeons need additional training to work with lymphatic vessels.
The rat model, which is commonly used for microsurgical training, is also useful to become familiar with lymphatic vessels.
Furthermore, for starting an individual experience in dealing with lymphatic collectors, this experimental model is easily accessible and can give answer to the level of the personal success rate for anastomosing lymphatic vessels.
Also for establishing the technique, the rat model was used to evaluate basic strategies in lymphatic vessel microsurgery.
2.1.1 Training to Suture Lymphatic Vessels on the Abdominal Thoracic Duct
For the first attempts of training, the abdominal thoracic duct may be appropriate.
Under general anesthesia, the rat, with an optimal weight of about 250 g, is fixed lying on the back. The abdomen is opened via an incision beneath the left costal margin or a midline incision. The intestine together with the spleen is rotated to the right side and fixed with broad hooks (Fig. 2.1). With the help of two Q-tips, which are rotated in contrary direction, the aorta is exposed.
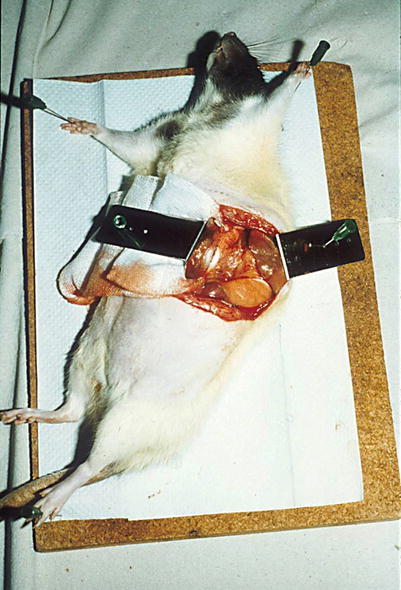
Fig. 2.1
Rat weighting around 250 g, the intestine together with the spleen is rotated to the right side and fixed with broad hooks; the left side of aorta is exposed
Just next to the aorta, the lymphatic abdominal thoracic duct is found on the left side. After a meal, the duct is seen as a milky structure filled with chyle. Otherwise it is recognized more difficulty just as a translucent structure.
The abdominal thoracic duct commences with the confluence of the lumbar and intestinal lymphatic ducts. On the way toward the diaphragm, it crosses the lumbar branches of the aorta. These should not get damaged because of possible bleeding. In between two branches, however, the abdominal thoracic duct is easily accessible (Fig. 2.2).
Fig 2.2
Access to the abdominal thoracic duct between the cisterna chyli and diaphragm between two lumbar branches for suturing and harvesting lymphatic segments for transplanting
In direction to the diaphragm, care has to be taken not to open it accidentally since a pneumothorax will result.
The thoracic duct is separated from the aortic wall in a blunt technique with gentle movements by closed forceps. The border toward the abdominal aorta becomes obvious, and a similar procedure can be performed from the opposite side of the vessel.
The longtime experience with lymphatic vessels showed that, despite the thin wall, the vessels are relative resistant against longitudinal tension forces. They can be pulled and transferred with gentle stress.
If however the vessels are opened and tension is applied to the vessel wall in oblique direction, the fragile wall is ruptured very easily.
Small vessels are often anastomosed using the technique of Cobbett (1967). With this technique, the vessel wall is turned around to facilitate the suturing of the back wall with the help of corner sutures which are put under tension during rotation. This turned out not useful in suturing lymphatic vessels, since the corner sutures, set under tension, ruptured the tiny wall. In longitudinal direction, however, the vessels as a whole are remarkable resistant against tension.
The so-called tension-free anastomosing technique minimizes the forces applied to the vessel wall in oblique direction. It starts with a corner suture opposite to the surgeon. The back wall then is just lifted as far as the needle needs space to fix the back wall on both sides with single stitches leaving the knot on the outer surface. By that way the vessel remains in place without being turned around. Suturing of the back wall is completed with the second corner stitch in front of the surgeon. The front wall is thereafter easily completed by single stitches (Figs. 2.3, 2.4, 2.5, and 2.6) (Baumeister et al. 1981a, b, c).
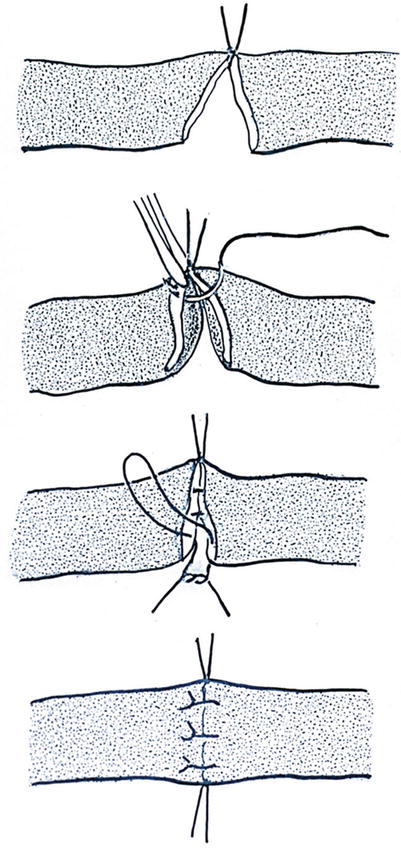

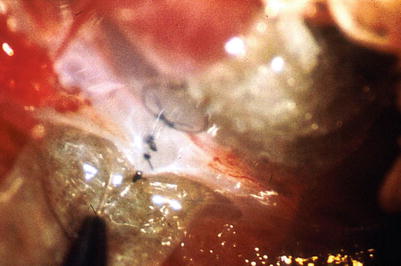
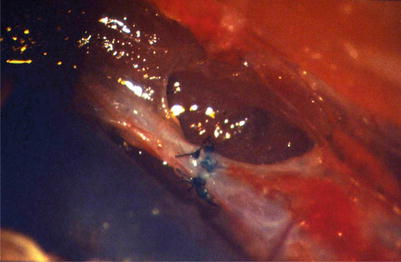
Fig. 2.3
Scheme of the “tension-free anastomosing technique,” avoiding tension also in oblique direction starting with the first corner suture opposite to the surgeon, back wall gently lifted for single sutures, second corner suture and completing the front wall, no turning the vessel (With permission Baumeister et al. 1981 b from Wiley global permission)
Fig. 2.4
First corner suture
Fig. 2.5
Back wall completed as well as the second corner suture
Fig. 2.6
Lymphatic vessel suture completed
For training, the vessel should not be transected completely at first since this would result in retraction of the two endings. The single stitches would have to be performed under tension. If however at least a small part of the wall remains, the suturing is possible without tension.
In the case of a complete transection, it is recommended to interpose a lymphatic segment, harvested from a second animal. The interposed segment has to be inserted in the right direction of the lymphatic flow (Figs. 2.7 and 2.8).

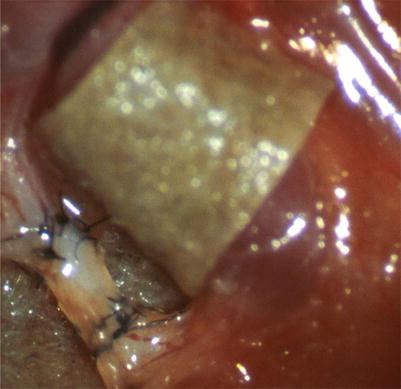
Fig. 2.7
Segment of the abdominal thoracic duct ready for grafting
Fig. 2.8
Interposed lymphatic segment at the abdominal thoracic duct next to the rat aorta (With permission Baumeister et al. 1981b, from Wiley global permission)
It also gives the possibility to check the behavior of grafting in principle together with checking two anastomoses in a row.
For exercising, it might be useful to perform as many stitches as it might be applicable. However in man the number of sutures should be limited because the lymphatic vessels in patients are often much smaller than the abdominal thoracic duct in rats weighting 200–300 g.
With more experience, also the lumbar lymphatic vessels may be used for training to suture smaller lymphatic vessels.
2.1.2 Experiments on the Abdominal Thoracic Duct
2.1.2.1 Patency and Suture Material
At the abdominal thoracic duct, the patency of the anastomoses (Baumeister et al. 1980; 1981b), the patency rate of grafts (Baumeister et al. 1980; 1981b), and the reaction on the suture material (Baumeister et al. 1982a) were studied.
The patency was examined by visual examination after injection of dye (Patent Blue V®) and by histological examination. Patent Blue V® has a high molecular weight and is specifically taken in by the lymphatic capillaries.
Additionally, patency and function were studied using isotopes.
As atraumatic and monofilament suture material, absorbable polyglactin 910 (Vicryl®, Ethicon) and nonabsorbable Polyamide 6.6 ®, (Ethicon) size 10-0 to 12-0 were used.
After a mean observation period of 65 days, all ten grafts were judged as patent by inspection during the reoperation.
In 9 out of 10 grafts, the dye appeared cranial to the transplants after injection in the cisterna chyli.
Also 9 out of 10 grafts were proved patent by histological examination. In the occluded graft, nonabsorbable sutures have been used.
Out of the ten transplants, five were sutured with nonabsorbable Polyamide 6.6 and 5 with absorbable polyglactin 910 (Table 2.1).
Table 2.1
Patency of autogenous lymphatic grafts in the rat abdominal duct
N = 10 | |
|---|---|
Evaluation method | Patency |
Inspection | 10/10 |
Dye injection | 09/10 |
Histology | 09/10 |
During the whole investigation period, a marked foreign body reaction was seen around the nonabsorbable sutures (Fig. 2.9).
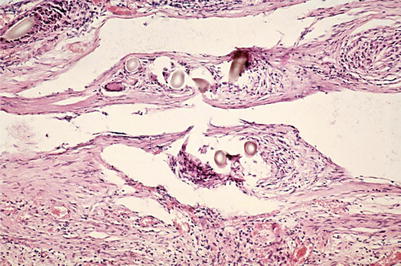
Fig. 2.9
Patent anastomosis of the abdominal thoracic duct, nonabsorbable suture material (Polyamide 6.6.), 8 weeks after surgery, marked foreign body reaction close to the vessel (H-E, tenfold magnification of objective)
On the contrary, the reaction around the absorbable sutures diminished with time after the operation. Just remnants of the material were seen as contents of foreign body giant cells (Fig. 2.10).
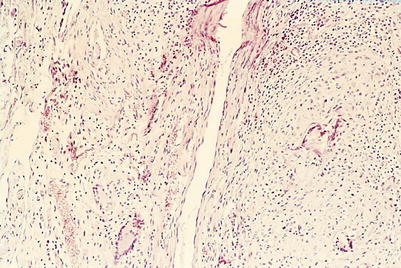
Fig. 2.10
Patent anastomosis of the abdominal thoracic duct, absorbable suture material polyglactin 910, 6 weeks after surgery, minor foreign body reaction (H-E, tenfold magnification of objective)
In summary, the diameter of the foreign body reaction of the nonabsorbable material was bigger than the lymphatic vessel diameter itself. Therefore we used absorbable material further on. Polyglactin 910 was available with a size of 11-0 until the process of production was altered. Nowadays only the size 10-0 is available.
Lympho-lymphatic anastomoses have been investigated also by electron microscopy. Electron microscopy investigations revealed a smooth inner surface at the site of the anastomosis. In Fig. 2.11, the area of a lympho-lymphatic anastomosis is opened by an oblique cut of the vessel. The nonabsorbable suture material marks the site of the anastomosis. The vessel is stabilized by a small round insert for the electron microscopy preparation. The anastomosis is patent, the inner surface is smooth, and the endothelial layer is continued from one vessel to the other (Fig. 2.11).
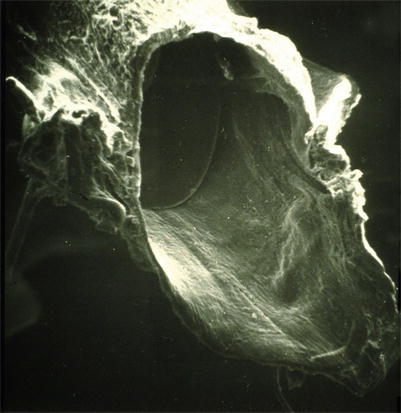
Fig 2.11
Scanning electron microscopy (oblique cut of the anastomosing site) 11 weeks after lympho-lymphatic anastomoses (nonabsorbable suture material), patent anastomosis, smooth inner surface continuous endothelial layer
2.1.2.2 Function of Grafts
Homologous transplantations of segments of the abdominal thoracic duct were performed on inbreeding Long-Evans and Lewis rats with an average weight of 250 g. The anastomoses were performed with the tension-free anastomosing technique.
The patency of the lymphatic grafts and the function as well were examined by injection of 131 I gamma globulin. The injection was performed within the cisterna chyli using an infusion pump. The activity was measured in the area above the thoracic duct in the chest (Fig. 2.12).
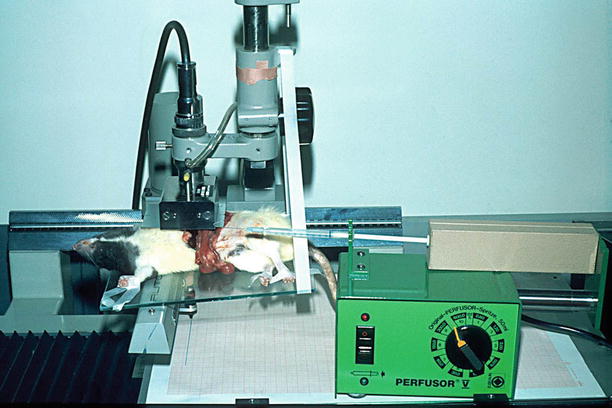
Fig. 2.12
Assessment of function after reconstruction of the abdominal thoracic duct by lymphatic grafts, injection of 131 I gamma globulin in the cisterna chyli, measurement above the thorax
In untreated animals, a quick rise of activity could be observed after the injection. After ligation of the thoracic duct beneath the diaphragm, no elevated activity was detected at the chest. After interposition of the transplants, a quick rise in activity was seen like in normal animals (Fig. 2.13).
Fig. 2.13
Measuring the activity of marked albumin at the chest after injection into the cisterna chyli (arrow, start of the injection). (a) Untreated animal. (b) After ligation of the abdominal thoracic duct beneath the diaphragm. (c) 8 weeks after transection of the abdominal thoracic duct and interposing a lymphatic graft (arrow, Injektionsbeginn: starting the injection) (With permission Baumeister et al. 1981b, from Wiley global permission)
2.1.2.3 Immunologic Behavior of Transplanted Grafts
Grafts of the abdominal thoracic duct in a length of about 3 mm were harvested in Druckrey-Berlin 9 (DB9) rats, and they were interposed in the corresponding area in an orthodromic direction in Long-Evans (LE) rats.
In order to prove the genetic difference, in 10 DB9 animals, full-thickness skin grafts were transplanted with a diameter of 16 mm to Long-Evans rats. The grafted skin was rejected in 9 out of 10 animals at day 14, in one animal at day 16.
The results of the allogeneic transplantation were compared to the isogeneic transplantation in Long-Evans rats (Baumeister et al. 1982a, b; Gabka 1983).
The groups consisted of 15 animals.
The patency of the grafts was examined by inspection and by dye injections.
Random samples of the transplants were investigated also by electron microscopy.
After a mean observation period of 67 days, 14 out of 15 grafts were rated as patent by inspection and by dye injection in isogeneic transplantation.
In homologous transplantation, 13 out of 15 grafts were proved as patent after a mean follow-up period of 60 days (Table 2.2).
Table 2.2
Patency of isogeneic and allogeneic transplanted segments of the abdominal thoracic duct in rats
Isogeneic transplantation | Allogeneic transplantation | |
|---|---|---|
Evaluation method | Mean observation period 67 days | Mean observation period 60 days |
Inspection | 14/15 | 13/15 |
Dye injection | 14/15 | 13/15 |
Between day 14 and 60 random investigations by electron microscopy were performed.
In normal abdominal thoracic ducts, the endothelium was smooth. The endothelial cells were closely connected, sometimes showing microvilli. Collagen fibers type I showed an exact arrangement in alternate directions. In between collagen fibers of type III were seen. Within the deeper layers of the lymphatic wall, fibrocytes, some capillaries, and single fat cells were seen.
In contrast, 14 days after allogeneic transplantation, no continuous endothelial covering could be detected. Instead, the inner surface was covered by a fibrous network. The formerly structured arrangement of collagen fibers was destructed. Collagen fibers type I and II were thus present on the inner surface.
Within blood-containing vessels, the collagen fibers type III would increase the risk of thrombosis. In lymphatic vessels, however, no significant thrombosis was seen. The reason for this might be that the potential of coagulation is reduced in lymphatic fluid to about one-third, and therefore no thrombosis was detected (Yoffey and Courtice 1970).
During weeks 3 and 4, a neointima started from the adjoining intact duct to cover the whole inner surface of the transplants. Blood capillaries grow in the vessel wall toward the neointima.
Between days 40 and 60, within the wall caverns appeared, together with a massive infiltration of activated lymphocytes, plasma cells, macrophages, and erythrocytes. The wall however remained stable because of the new endothelium and the subendothelial tissue containing a continuous basal membrane, structured collagen fibers type I, and differentiated muscle cells (Figs. 2.14, 2.15, and 2.16).
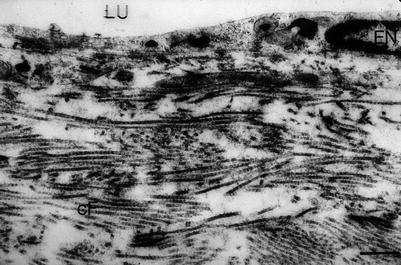
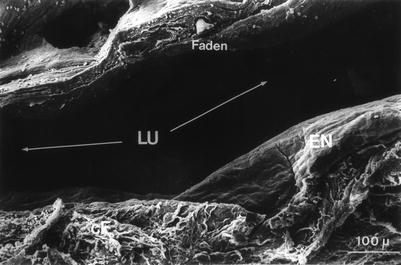
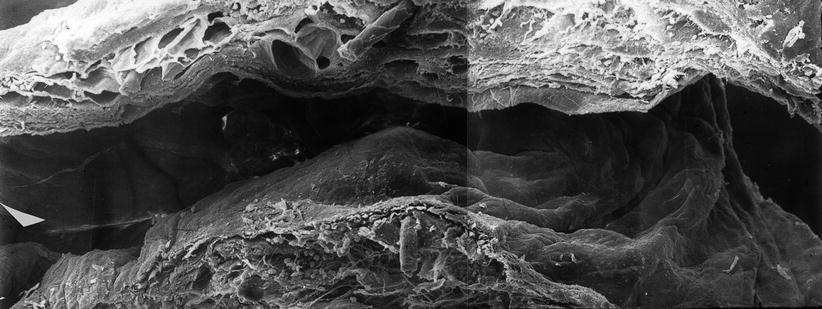
Fig. 2.14
Allogeneic abdominal thoracic duct graft of rat. 40 days after grafting (ultrathin section, 1000-fold magnification) (E endothelial cell, LU lumen, cF collagen fibers)
Fig. 2.15
Allogeneic abdominal thoracic duct graft of rat. 40 days after grafting (scanning electron microscopy, 440-fold magnification). LU lumen, EN endothelium, cF collagen fibers, Faden suture)
Fig. 2.16
Allogeneic abdominal thoracic duct graft of rat 60 days after grafting (scanning electron microscopy, composition 700-fold magnification), site of anastomosis, graft left, host-vessel right
In summary, allogeneic transplantation of segments of the abdominal thoracic duct from DB9 rats to LE rats showed a high long-term patency rate similar to that seen in isogeneic transplantation. Investigation by electron microscopy showed an immunologic reaction, first at the endothelium and later in the deeper areas of the vessel wall. This did however not cause a destruction of the transplant and interfere with the function. The low pressure within the lymphatic transporting system and the low coagulability of lymphatic fluid might be the reasons for these surprising findings.
Related posts:
 Reconstructive Lymph Vascular Surgery and Other Lymphedema Treatment Modalities
Reconstructive Lymph Vascular Surgery and Other Lymphedema Treatment Modalities
 Pathophysiology of Lymphedemas with Respect to Surgery
Pathophysiology of Lymphedemas with Respect to Surgery
 Methods for Objectification of the Results
Methods for Objectification of the Results
 Indication and Technique of Reconstructive Lymph Vascular Surgery
Indication and Technique of Reconstructive Lymph Vascular Surgery
 Results of Reconstructive Lymph Vascular Surgery
Results of Reconstructive Lymph Vascular Surgery
 15: Hand Cleansers and Sanitizers
15: Hand Cleansers and Sanitizers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


