Expanding the applications of radiofrequency dermatologic surgery
Radiofrequency (RF) surgery is a versatile tool. With experience you will be able to expand the applications of radiofrequency surgery by making full use of the set of electrodes provided with the equipment by the manufacturer. As you work more with the machine, you can develop more applications taking into account the histopathology of skin conditions, the electrodes, the waveforms, and power. In all applications, the art of the use of electrodes will always make a great difference as far as the cosmetic outcome is concerned.
Table 14.1 contains some of the common applications that I later developed. In addition to applications in Table 14.1, there are few more that though not commonly done still show the versatility of radiofrequency surgery. Please refer to Table 14.2 for details.
Skin lesion | Waveform | Electrode | Power |
|---|---|---|---|
Molluscum contagiosum | RFD | S/B | 1–2 |
Syringoma | RFD | S/B | 1 |
Senile comedones | RFD | S/B | 1 |
Closed comedones (whiteheads) | RFD/RFE | S | 1 |
Xanthelasma | RFD | S | 1 |
Cherry angioma | RFD/RFC | S/B | 1 |
Earlobe repair | RFE | TW | 3 |
Mucocele | RFB | S/L | 3–4 |
Capillary hemangioma | RFB and RFC | L and B | 3–6 |
Pyogenic granuloma | RFB and RFC | L and B | 3–6 |
Trichoepithelioma | RFE | L | 3–4 |
Neurofibroma | RFE | L | 3–4 |
Cutaneous horns | RFE | S/L | 3–4 |
Keratoacanthoma | RFE | L | 3–4 |
Freckles | RFE | S | 1 |
Mucosal lesions (warts, fibroma, etc.) | RFE/RFB | L/T | 3–5 |
RFD | S/D | 1–2 |
Notes: RFE, radiofrequency excision (cut) waveform; RFB, radiofrequency blend waveform; RFD, radiofrequency desiccation waveform; RFC, radiofrequency coagulation waveform; S, straight needle electrode; L, round loop electrode; T, triangular electrode; B, ball electrode TW, thin wire electrode; D, broad needle electrode.
Skin lesion | Waveform | Electrode | Power |
|---|---|---|---|
Hypertrophic scar/keloid | RFE/RFB | S and L/T | 3–8 |
RFC | B | 5–10 | |
Condyloma acuminata | RFE/RFB | L/T | 3–4 |
RFD | S/D | 1–2 | |
Genital lesions | RFE/RFB | L/T | 3–4 |
RFD | S/D | 1–2 | |
Periungual and subungual lesions | RFB | S and L | 3–8 |
RFC | B | 6–10 | |
Ingrown toenail | RFC | M | 5–6 |
Rhinophyma | RFE | L | 3–5 |
Gray facial hair | RFC | H | 1 |
Chronic lichenified eczema | RFB | L | 3–6 |
Prurigo nodularis | RFB | L | 3–6 |
Hypertrophic lichen planus | RFB | L/T | 3–6 |
Any papular or nodular lesion of unknown etiology | RFE/RFB | L/T | 3–6 |
Telangiectasia | RFC | STE | 1 |
Basal cell carcinoma | RFE/RFB | L | 3–6 |
Notes: RFE, radiofrequency excision (cut) waveform; RFB, radiofrequency blend waveform; RFD, radiofrequency desiccation waveform; RFC, radiofrequency coagulation waveform; S, straight needle electrode; L, round loop electrode; T, triangular electrode; B, ball electrode; M, matrixectomy electrode; H, hair-removing electrode (insulated), three sizes; STE, special telangiectasia electrode TW, thin wire electrode; D, broad needle electrode.
I will be touching upon a few selected applications to highlight the practical points while dealing with them.
Molluscum Contagiosum
Molluscum contagiosum is a very common viral infection that needs urgent treatment because of its potential to spread to other areas. Though commonly seen in children, its incidence in adults has significantly increased. Nowadays, we encounter many cases of “giant” molluscum in adults and occasionally in children as well. In children, the face and neck are very commonly affected, whereas in adults, the face, genitals, and groins are commonly affected. See Figures 14.1 to 14.4.

Figure 14.1Molluscum contagiosum near eye.

Figure 14.2Molluscum contagiosum near eye were electrodesiccated under local anesthesia.

Figure 14.3Giant molluscum contagiosum over neck and chin in a child.

Figure 14.4Clean excision of giant molluscum contagiosum was done under short general anesthesia in operation theater.
All molluscum lesions are best treated using the desiccation method.
I prefer a straight needle electrode or even a thin wire electrode for tiny and small lesions on a child’s face. A broad needle electrode may be used in bigger lesions.
As described earlier, desiccation whitens the lesions due to dehydration and the molluscum body also is coagulated and necrosed due to heat generated. There is no need to enucleate a molluscum body; it gets necrosed and blends with the scab of desiccation to peel off within a week.
Large or giant molluscum are best excised under local anesthesia.
Multiple molluscum on the face, genitals, and groin are best treated under surface or topical anesthesia.
Multiple molluscum in children can be treated in a single session in the operation theater under short duration general anesthesia; done as a “daycare” procedure.
Immune status needs to be investigated in case of multiple molluscum in adults, especially to rule out HIV infection.
All treated patients must be followed up for recurrence and reinfection, which is very common, and counseling must be done beforehand to emphasize this.
Chances of scarring are negligible.
Syringomas
Syringomas are small superficial lesions arising from the eccrine glands and they commonly present around the eyes causing cosmetic disfigurement. See Figures 14.5 to 14.7.
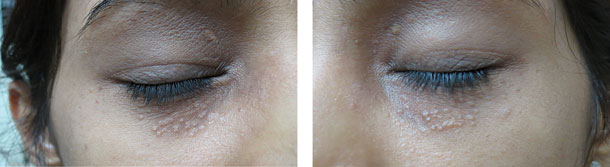
Figure 14.5Syringoma.

Figure 14.6Immediately after electrodessication of syringoma.

Figure 14.7Two months after electrodessication of syringoma (almost cleared).
Syringomas are difficult to treat in one session.
I treat multiple lesions in two to four sessions at fortnightly intervals.
Only soft-touch desiccation should be done without overlap.
Overzealous treatment may lead to hypo- or hyperpigmented scarring.
Some lesions may not respond in spite of proper treatment.
Recurrence is always possible, so patients should be aware of that.
Senile comedones
Senile comedones are very superficial lesions and commonly grouped over the nose, eyelids, and cheeks. The blackheads can be easily expressed out with a comedone expressor, but recur quickly. See Figures 14.8 and 14.9.

Figure 14.8Senile comedones in ear.

Figure 14.9Senile comedones immediately after electrodessication.
Single session treatment.
Surface or local anesthesia.
Soft touch desiccation is best.
All lesions will fall off within one week.
Generally no possibility of scarring.
Closed Comedones
Some patients of acne have numerous closed comedones on the face. These lesions can be stubborn to applications of topical retinoid and chemical peels. These lesions cannot be expressed out.
These lesions respond very nicely to the radiofrequency method.
It is advisable to use the cut waveform, thin wire electrode, with a power of 1 for very tiny lesions to minimize lateral heat damage on the face.
Overall, use of a straight needle electrode at a power of 1 with a desiccation waveform is best with very soft touch treatment.
I prefer treating multiple lesions in two sessions spaced at a fortnight interval.
All lesions clear within a week. There could be dyschromia but clears eventually with bleaching creams.
Xanthelasma
Xanthelasma lesions affect the upper and lower eyelids and are unsightly. All patients are advised to get a lipid profile done before surgery to find out if they have deranged lipids like cholesterol. This is not a rule. See Figures 14.10 and 14.11.

Figure 14.10Xanthelasma on upper eyelids.

Figure 14.11Xanthelasma immediately after treatment using electrodessication or electrosection at power 1.
The electrodessication method works out best here, because the lesions are very superficial and the eyelid skin is very thin.
I sometimes use the cut waveform at a power of 1 to have the least lateral tissue thermal damage to critically thin eyelid skin. The straight needle electrode is best.
Whatever method applied, care should be taken not to cause overlap.
Larger lesions are treated in more than one session at fortnightly intervals.
Cherry Angiomas
Nowadays, many patients demand removal of cherry angiomas. These are distributed over the arms, trunk, and face, and are small (1–5 mm). These are benign growths from skin capillaries. Treatment is purely for cosmetic reasons.
Waveforms of electrodessication or electrocoagulation can be used at a power of 1.
A ball electrode can coagulate the lesion fully within a second.
I use a straight needle electrode for smaller lesions.
The scab thus formed clears off within a week.
Scarring is unlikely.
Earlobe Repair
Demand for earlobe repair has increased in all age groups with the increasing use of fashionable ear ornaments. There could be incomplete (partial), complete, or multiple tears. See Figures 14.12 to 14.16.

Figure 14.12Ear lobe before treatment.

Figure 14.13Ear lobe repair done using tissue glue.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


