Dorsal preservation (DP) rhinoplasty is a surgical technique designed to modify the nasal dorsum without disrupting the keystone area, offering a natural and long-lasting outcome. Unlike traditional methods that require reconstruction of the middle vault, DP preserves structural continuity, reduces the need for grafts, and minimizes long-term irregularities. Ideal candidates have a thin, regular dorsum and strong cartilage, though advances in tools like piezoelectric instruments have expanded its applicability to patients with wider, irregular dorsums. The technique involves precise nasal and septal modifications. DP is increasingly favored due to its efficiency, improved outcomes, and growing adaptability to diverse nasal anatomies.
Key points
- •
Dorsal preservation rhinoplasty: A technique preserving nasal structure by avoiding middle vault disruption, ensuring natural, long-lasting results with fewer grafts and complications.
- •
Advances in instruments: Modern tools like piezoelectric devices have expanded dorsal preservation (DP) applications, enabling precise fractures and cartilage reshaping for diverse nasal anatomies.
- •
Tailored techniques: DP methods (eg, septal pyramidal adjustment and repositioning [SPAR] A, B, and C) are customized to patient needs, addressing dorsal reduction, elevation, or deviation correction effectively.
- •
Ideal candidates: Best suited for patients with thin, regular dorsums and strong cartilage, but adaptable for broader indications due to surgical innovations.
- •
Minimized complications: Improved understanding and instruments reduce risks like hump recurrence, radix step, and supratip saddling, ensuring reliable, esthetic outcomes.
Introduction
Dorsal preservation (DP) was first described in 1899 by Goodale, and a lot has changed since then. It is any technique of moving the dorsum (up or down) that does not open the cartilaginous middle vault, in other words, does not disarticulate central keystone area. It is the opposite of the traditional dorsal dehumping that typically involves opening the middle vault and rebuilding it with spreaders grafts/flaps.
This technique has re-emerged as an important option for managing the dorsum and is changing the way rhinoplasty is performed. It is apparent that the trend is toward preservation of the structure to provide a natural and long-lasting outcome.
The advantages of DP (compared to structured dorsal rhinoplasty) are that it is a faster surgery, with no necessity of rebuild middle third, with less grafts and irregularities in long term, leading to a more natural result. In other words, keep the continuity of bone and cartilaginous vault in the middle line. The disadvantages include necessity of better control of bone structures and precision fractures.
Like any other surgical technique, DP rhinoplasty has its indications and limitations. In this article, we focus on showing the different PD techniques and their approaches, our personal strategies and results, as well as a literature review.
Methods
This is an original, descriptive article, based on the authors’ opinion to describe a surgical approach for the esthetic-functional correction of nasal deformities.
To prepare this article, a review of medical literature, in English, Spanish, and Portuguese, was carried out on topics related to rhinoplasty, in addition to the report and experience of the authors who use such techniques routinely in their services.
Pure dorsal preservation
DP resurged as an alternative to traditional dorsum resection with reconstruction in the last few years; it is seen as more natural and with better long-term results. It has been practiced for more than 120 years in some specific centers around the world and has gained interest in recent years in view of the improvement of the instruments and techniques that enable it to be carried out.
The classic main indications of DP are thin dorsum, strong cartilages, and regular dorsum, and the contraindications is the opposite, that is, irregular and wide dorsum and weak cartilages. Much of the interest in DP is due to the avoidance of the potential negative implications of excisional techniques. The maintenance of the structural integrity at the nasal keystone, dorsal esthetic lines, and the patency of the internal nasal valve are some of the positive points of DP.
There are mainly 2 basic principles of DP: nasal fractures and septoplasty. All techniques can be carried out by either an open or a closed approach; after exposure of the osteo-cartilaginous skeleton, it is necessary to do submucosal dissection of the nasal septum.
To have impaction of the nasal pyramid, it is necessary to disarticulate the nose from the face; to achieve this, it needs to perform complete lateral and transverse fractures. Lateral fractures can be just a simple osteotomy (described as “push-down”) or removal of a bone fragment/ostectomy (described as “let-down”). The transverse fractures must be complete and are performed in the position where the new radix is desired.
To perform fractures in the nasal bones, for a long time we only had osteotomes, chisels, and saws. Although they are excellent instruments, they are not very precise, with the risk of comminution and multiple fractures of the bones, leading to loss of control over the projection of the nasal pyramid.
The only technique described for a long period for modifying the nasal septum were the removal of the lower strip. , The other techniques for removing the high and intermediate strip are described more recently in the literature and have been adding to and improving the indications for DP. , ,
Because of the difficulty of the fractures and the few alternatives for changing with the nasal septum, DP led to some stigmas, which caused several surgeons to abandon this technique. The main complications are radix step, infantilization of the nose, supratip saddling, hump recurrence, and widening of the nasal pyramid—we will describe each one in later discussion.
Modern dorsal preservation
With the advent and improvement of knowledge of anatomy of the nose, and the instruments such as the piezo and drill, DP has seen a resurgence in recent years (specifically since 2019). Techniques have evolved, and complications that were previously common no longer occur.
There are several DP techniques described in literature, but we decide which depending on the amount of dorsum reduction, high of radix, dorsum centralization (or not), and septal deviation. We always use the easiest technique to the most complex: surface greater than SPAR A greater than SPAR B; the differences between them are mainly septoplasty strip removal. In cases that we want to raise the dorsum, we use SPAR C (divided into SPAR C/A and SPAR C/B)—we will describe each technique in the following sections.
Patient selection
Ideal patients have a thin and regular dorsum (V-shaped) and strong cartilages. A thin dorsum is a classic indication of DP; however, with the use of the powered instruments, it is possible to make the dorsum thinner without opening the nasal valve and then to expand our indications and the variety of patient that can benefit from the technique.
The shape of the dorsal convexity is very important in selecting good candidates for DP techniques. A V-shaped hump has only 1 curvature (dorsal profile angle), which can be more readily flattened, whereas an S-shaped hump has 2 curvature points (dorsal profile angle and kyphion angle) and is more difficult to flatten, this one is much more common (88%). By using preservation techniques in appropriate candidates, the likelihood of success will be higher.
The importance of strong cartilages is because the nose will be supported by 2 main points: the perpendicular plate of the ethmoid (PPE) and the nasal spine (NS). If the cartilages do not have enough tension, the nose may lose projection or even become crooked. A solution in cases of weaker cartilages, in the most caudal portion of the nose, would be to support the dorsum using rib.
Lateral fractures
After opening and exposing the nasal structures, we generally initiate with lateral fractures. We always perform the use of the piezo in the naso-facial groove (lower portion of the frontal process of the maxilla). If the planning is lowered until 2 mm of dorsum, we only perform simple fractures (“push-down”). If we want to dehump more than 2 mm, we perform an ostectomy (“let-down”) in a shape of “banana” or “boomerang.”
This ostectomy must be proportional to the amount that we will dehump the dorsum; a simple scale will leave 2 mm extra due the in-fracture. For example, if we want to dehump 5 mm of the dorsum, we remove 3 mm of bone fragment (the remaining 2 mm will enter in the piriformis fossa due to in-fracture).
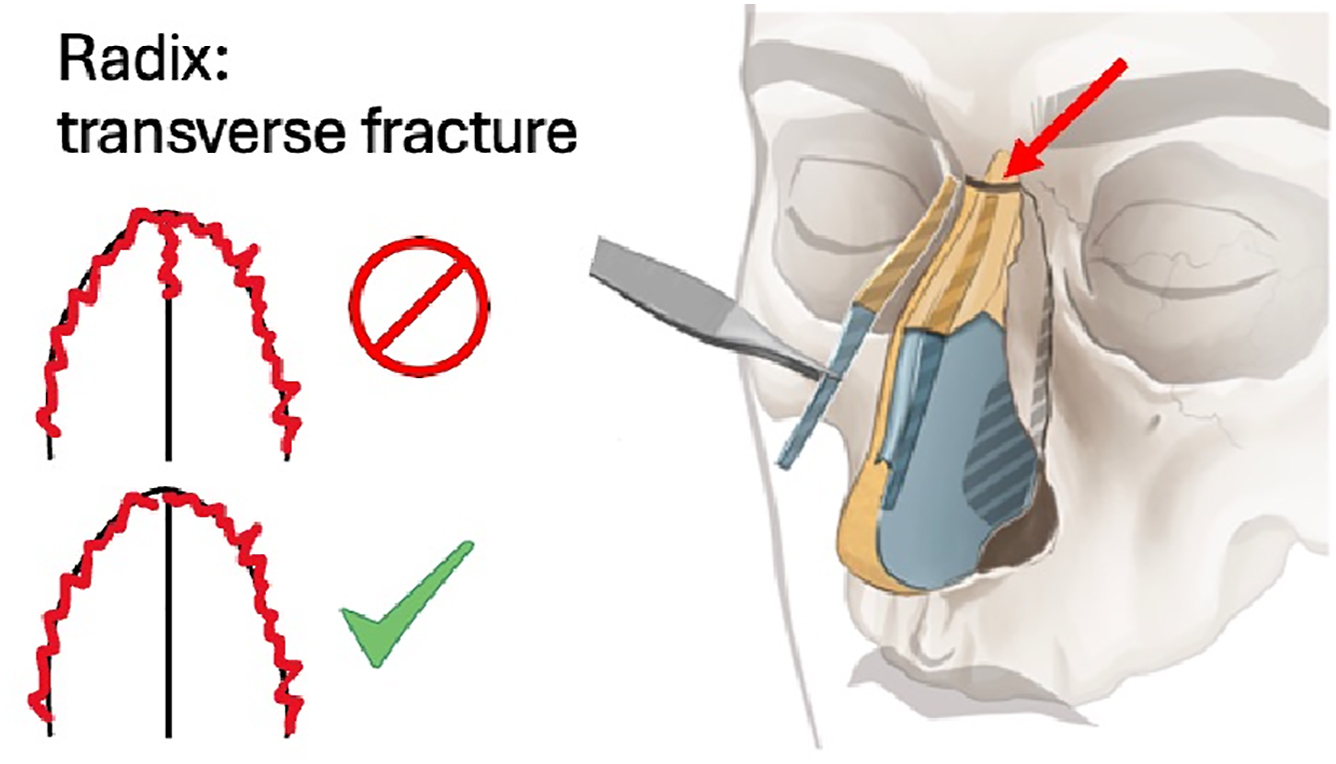
Transverse fractures
Transverse fractures are the ones we must be most careful. With piezosurgery, they become more precise, and in this way, we have more control at the radix. An inadvertent fracture of PPE can lead to loss of control of the height of the radix and consequent infantilization of the nose, as well as radix step. This was a frequent complication that occurred with osteotomes, and which improved significantly with the use of piezo.
Remembering that the site of the transverse fracture will be the new radix; therefore, we suggest always making it as cephalad as possible. Making it more caudal can lead to the same risks, such as the formation of a step and infantilization of the nose.
When performing these fractures, it is very important not to enter with the piezo insert all inside the bone; in another words, just cut the outer layer of the nasal bone. Often the PPE is fused to the nasal bone, and deep insertion of piezo’s insert may lead to inadvertently cutting the PPE. We must respect PPE as the height of the radix must be controlled by the work on the PPE, not by the fractures ( Fig. 1 ).
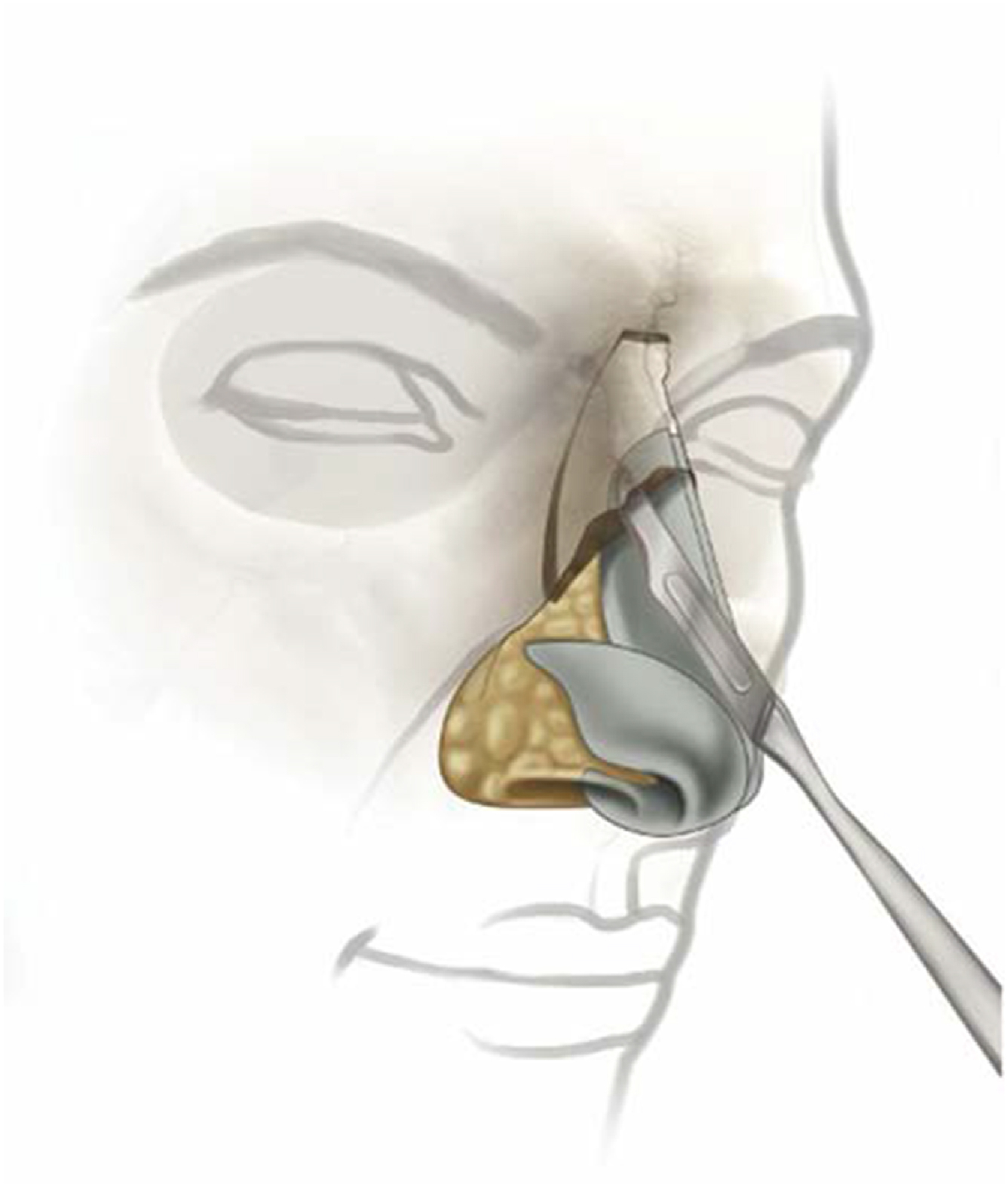
Lateral split/ballerina maneuver
This maneuver, which is nothing more than the disarticulation of the upper cartilage of the nasal bone, aims to facilitate the improvement of the shape of the nasal dorsum. It aims to transform a convexity into a concavity, that is, a hump into a straight or slightly curved dorsum. By disarticulating the nasal bone from the upper cartilage and piriform ligament, there is a reduction in tension in this area, making the dorsum smoother ( Fig. 2 ).
Related posts:
 Understanding Dorsal Preservation Rhinoplasty
Understanding Dorsal Preservation Rhinoplasty
 Preservation Rhinoplasty—Outcomes in Dorsal Preservation Rhinoplasty
Preservation Rhinoplasty—Outcomes in Dorsal Preservation Rhinoplasty
 Subdorsal Flaps in Dorsal Preservation
Subdorsal Flaps in Dorsal Preservation
 The Fusion Sling—Revisiting the Nasal Tip Suspensory Anatomy
The Fusion Sling—Revisiting the Nasal Tip Suspensory Anatomy
 Spare Roof Technique A and B – A Step-by-step Guide to Avoid Suboptimal Outcomes
Spare Roof Technique A and B – A Step-by-step Guide to Avoid Suboptimal Outcomes
 Dorsal Augmentation with Preservation Concepts
Dorsal Augmentation with Preservation Concepts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


