CHAPTER 24 Expanded Uses of BTX-A for Facial Aesthetic Enhancement
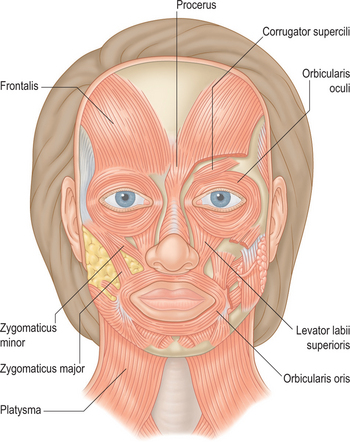
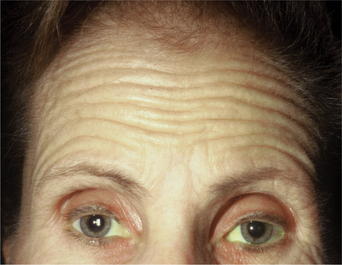
First described in the medical literature in 1992,1 the cosmetic use of botulinum toxin (BTX) has widened to include many previously inconceivable applications. Prior to this discovery, clinical experience with the use of the toxin was primarily limited to an option for the treatment of strabismus and a variety of disorders of chronically increased skeletal muscle tone2 (Fig. 24-1). The application of the toxin for aesthetic improvement was derived from keen observation of the appearance of facial soft tissue in patients who received the drug for a spectrum of disorders related to facial dystonia (Fig. 24-2). The toxin has become not only the gold standard in non-surgical facial rejuvenation, for eradicating dynamic rhytides in the forehead, glabella, around the eyes, and in the lower face and neck, but it has also become a viable alternative, as well as partner to surgery, for facial shaping and contouring.3,4 With essentially no downtime and few complications or adverse effects, the application of BTX in the environment of a comfortable clinical setting, represents the most modern form of cosmetic enhancement that is time-sensitive, safe, and effective (Fig. 24-3).



Treatment of the upper face and periorbita
A number of clinicians, impressed by the toxin’s obvious benefits and high level of safety, experimented with BTX for facial rejuvenation in the late 1980s, prior to the first reports published in the early 1990s.5,6 Although it appears obvious now that cosmetic improvement can be easily afforded by precision application of this agent for dozens of applications, initial enthusiasm was quelled by a lesser understanding of the various causes of facial aging and the possibilities for the use of this drug. Initially used primarily for the treatment of glabellar rhytides, BTX is now a first-line treatment for a number of cosmetic concerns, particularly in the upper face.7–21 To date, the three most common areas treated are the glabella, forehead, and lateral canthus for the treatment of rhytids in the respective regions. Treatment can be applied in various combinations to achieve the desired effect.
Glabellar rhytides
Historically, the ‘glabella’ was the area first and most described as a potential treatment site with BTX for aesthetic enhancement. Currently (at the date of publication) it is still the only facial site with FDA approval for the cosmetic use of BTX, specifically Botox Cosmetic. All other areas for which the toxin is used for cosmetic enhancement are considered ‘off-label.’ This means that under the physician’s discretion it is lawful to apply the drug in other areas with, of course, the appropriate patient consent. The glabella is loosely defined as the region depicted by the smooth elevation of the frontal region just above the bridge of the nose that extends laterally to each side onto and just above and lateral to the medial (head of) the eyebrow. The ‘glabellar complex’ often refers to a group of brow-associated muscles (mostly depressors in action) that function primarily for facial expression (Fig. 24-4). Muscles of the glabellar complex include the corrugator supercilii, procerus, depressor supercilii, and orbicularis oculi. Vertical glabellar frown lines arise naturally from the repeated activity of the corrugator supercilii and medial orbital orbicularis oculi muscles (plus depressor supercilii muscles) that not only induce vertical descent of the medial eye brow but cause adduction and depression of the surrounding soft tissue (Fig. 24-5).

Horizontal lines at the proximal nasal bridge typically located at the most caudal aspect of the glabellar complex are a manifestation of the muscular activity of the procerus and depressor supercilii muscles (Fig. 24-6).

In 1992, Carruthers et al injected 18 patients with BTX-A for the treatment of glabellar frown lines.1 Sixteen of 17 patients followed showed improvement for varying lengths of time with few side effects. This initial paper sparked a frenzy of interest across the globe. Following a number of publications, two randomized, placebo-controlled studies involving 537 patients confirmed the impressive safety and efficacy of the injection on the glabella. This led to the Food and Drug Administration (FDA) approval of BTX-A for the treatment of glabellar lines in 2002.22–24 This region has still been the most readily adopted area for the use of BTX for a variety of reasons mentioned previously, as well as a lack of consistent prior effective treatment options.
Dosing
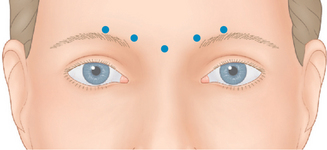
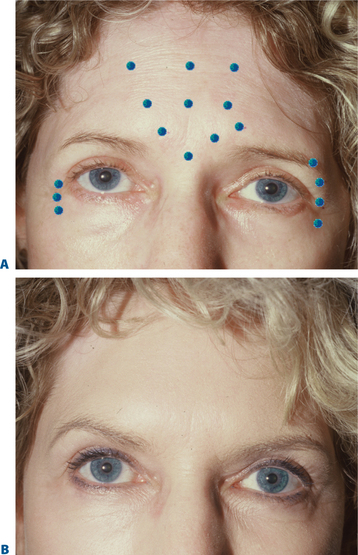
The strength and size of the muscles of the glabellar complex varies significantly from patient to patient. More importantly, despite similar anatomic components in most of us, a greater variable is the individual dynamics (i.e. the way we use our muscles). Although the most common treatment pattern utilizes two injections to each corrugator and one centrally to reduce procerus function (Fig. 24-7), individualizing treatment sites and doses to each patient will optimize clinical benefits. In addition, the exact effect desired may vary as well. In women, recent studies also suggest that higher doses may be longer lasting and give greater aesthetic benefit. A prospective, randomized, dose-ranging study of 80 women showed the greatest responses with the longest duration on glabellar lines with 30 and 40 U BTX-A, compared to the responses seen with only 10 or 20 U.25,26 Moreover, higher doses (20–40 U) produce an additional benefit of eyebrow lift.27 The likely cause for this effect resides primarily in the fact that with higher doses to the glabella region, there is enhancement of diffusion to the adjacent frontalis muscle.28 With this phenomenon, attenuation of the central frontalis activity by BTX induces a secondary hyperdynamic contraction/recruitment of the untreated lateral and superior frontalis that yields this effect (Fig. 24-8). In addition, the desired effects will vary from individual to individual as well. For instance, some individuals might have a more elevated medial eyebrow and prefer a greater lateral arch (Fig. 24-9). Precise and isolated injection placement of toxin to the corrugators and secondary brow depressors (typically a more caudal placement of the injection at or about the brow cilia) could further elevate the medial eyebrow reducing any chance of enhancing the desired brow contour. In these individuals, a ‘high-glabellar’ technique (Fig. 24-10 and DVD) might be preferable. This will affect both the brow depressors and adjacent frontalis muscle, and will reduce the glabellar vertical frown lines as well as induce a varying degree of medial brow descent. This will also be influenced by additional injections (or not) to the more cephalad portions of the forehead and dose (discussed below) (Fig. 24-11).

In general, men have a larger glabellar muscle mass compared with women. Studies comparing the efficacy and safety of the ranges of 20 to 80 U of BTX-A in men suggest that patients injected with doses as high as 80 U achieved a ‘better’ response rate than those injected with lower doses, without experiencing an increase in adverse effects.29 This high level dosing produces enhanced efficacy as well as persistence of effect which are not only required due to the greater muscle mass in males, but are also better suited to the male’s gender aesthetics and attitude. As in all treated areas, the most effective applications are delivered with precise injection techniques.
The most effective format of application and technique to this region has generated healthy debate. As in most facial regions, precision (i.e. targeting the recipient muscle with exactitude) will yield the most predictable responses. Understanding underlying facial muscle anatomy allows precision as to how much toxin is injected and where it is injected. The corrugator muscles lie deep to the insertion of the frontalis muscle in this region and just superficial to the periosteum of the supraorbital rim. Superficial injections (intradermal, subdermal/subcutaneous) will very likely equally (if not more) affect the frontalis muscle and will depend on diffusion to arrive at the corrugator muscles. Deeper injections (into the belly of this large muscle) will more accurately affect the corrugators in isolation. However, it should be mentioned that two of the authors (AC and JC) performed an objective study on 24 women with asymmetric medial eyebrows using an asymmetric injection technique as described above. On objective photographs taken at rest (Canfield system) there was no differential change in eyebrow height demonstrated. The techniques of one of the authors (SF) to this region is as follows (Fig. 24-12 and see DVD): The injector uses the non-dominant hand to stabilize the eyebrow between the thumb and forefinger and can also easily distract the medial eyebrow above the orbital rim. At the same time the injector can place the thumb into the supraorbital notch to protect against toxin migration posteriorly into the orbit. The injecting hand then orients the syringe at 90 degrees to the skin surface and with a swift motion attempts placement of the needle tip into the mid-aspect of the muscle in two places (the lateral and medial components of the corrugators). This maneuver is then repeated on the opposite side. Care is also taken to avoid unnecessarily puncturing periosteum (as happened with techniques described in the past, which aimed to pass the needle to the periosteum, then withdraw slightly to the muscle) as this can be a cause of headache and post-injection pain, probably due to periosteal inflammation.

Finally, this section would be incomplete if there were not a mention of our aesthetic goals that include what constitutes a satisfactory endpoint and outcome with effective dosing. Unfortunately, the concept of ‘immobility’ has become, in the mind of some consumers, synonymous with ‘effective’ treatment. Patients will return to your office to display their ability to ‘frown’ with the most unusual and noble efforts that produce the vaguest glimmer of a vertical frown line (Fig. 24-13). As in most situations, educating your patients on what they should expect and what constitutes an aesthetic satisfactory result that might not include immobility will avoid many phone calls and return visits and ultimately a happier and well-informed patient.

Horizontal forehead rhytides
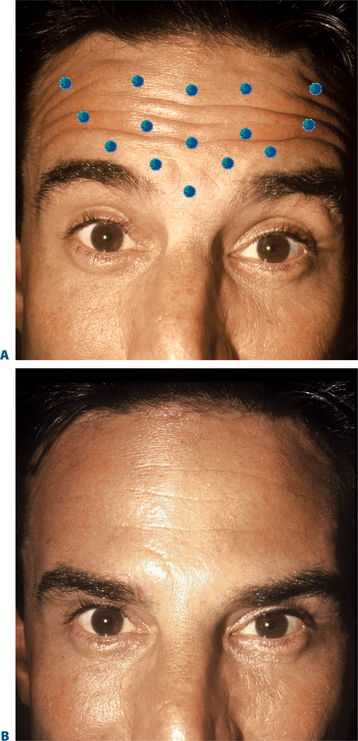
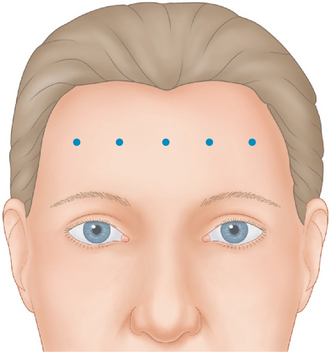
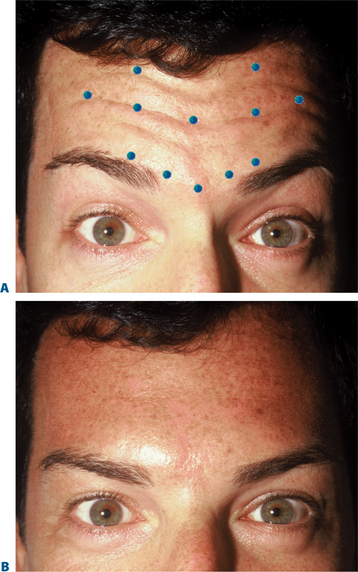
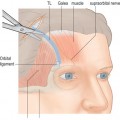
The frontalis is a large, quadrilateral muscle that originates in the galea aponeurotica. It inserts inferiorly into the procerus, orbicularis oculi, depressor supercilii muscles and anteriorly over the corrugator supercilii muscle, and terminates beneath the skin of the eye-brow. Although most figures (Fig. 24-4) depict the frontalis in two sections, it usually spans the forehead from one temporal fusion line to the other and may be thicker in certain portions of the forehead. The frontalis raises the eyebrows and skin over the root of the nose and also draws the scalp forward. Contraction of the frontalis primarily produces a series of horizontal forehead wrinkles and furrows. The most active portion of the frontalis muscle in most individuals is the 2 or 3 cm immediately above the brow. Activity in this portion produces horizontal rhytids that can appear as cephalad as the anterior hairline (Fig. 24-14). This finding is important when deciding at what locations BTX will be injected for a particular individual. Also, the effects of inducing brow ptosis will be greater if the lower portion of the forehead is injected (Fig. 24-15). In many individuals, a single row of treatment sites in the midforehead is effective in reducing or eliminating rhytids while preserving brow position (Fig. 24-16). Finally, as with most areas of the face, individual unique habitual animation and the desired aesthetic effects will dictate where the drug is applied. The lateral extent of the forehead injection sites will be influenced by a com-bination of aesthetic desires and the functional anatomy.
BTX-A injected across the forehead lessens undesirable horizontal forehead lines for a period of 4–6 months.30 Although treatment is individualized for each patient, in most individuals injections should be placed 2.5–3 cm above the brow proper to avoid brow ptosis or a lack of natural expressiveness. In general, narrow brows receive fewer injections and lower doses than broader higher brows. The exact site and dosage will depend on each individual presentation and the desired effects.
Dosing
As in the glabella, prior research suggested that higher doses of BTX-A may be more effective than lower doses in the forehead. A randomized, double-blind, dose-ranging study examined 60 women injected with either 16, 32, or 48 U BTX-A in eight sites and found the greatest improvement and duration of response with 48 U.31 However, adverse effects (headache, eyelid swelling, and brow ptosis), though uncommon, were more frequently associated with the higher doses. For reasons less clear that might relate to muscle mass, the number of active neuromuscular junctions is less in the frontalis muscle,32 BTX-A effects in this region (for any combination of the postulated causes), usually last longer than any other facial area. Therefore despite a slight reduction in regional efficacy, lower dosages (and few injection sites) may allow for a more harmonious onset and dissipation of effects. Retained animation, reduction in the degree of induced brow ptosis and greater aesthetic benefits also result from more conservative dosing (Fig. 24-17). As mentioned, the frontalis is unusually ‘sensitive’ to even seemingly low doses of drug. The placement (whether intradermal, immediately subcutaneous, deep subcutaneous, or intramuscular) has less bearing on the result. Although a direct intramuscular injection usually gives the most effective treatment, the authors advocate a more superficial injection that helps avoid bleeding, bruising, significant pain, or hematoma that can ‘spoil’ an otherwise perfect application in selected individuals.
Brow lift and contouring
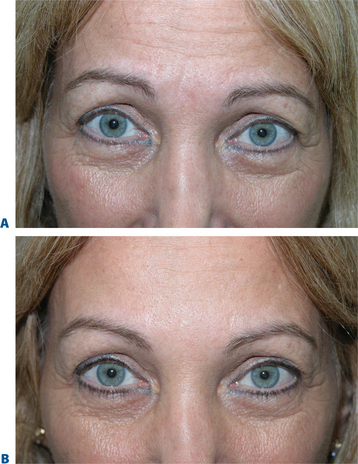
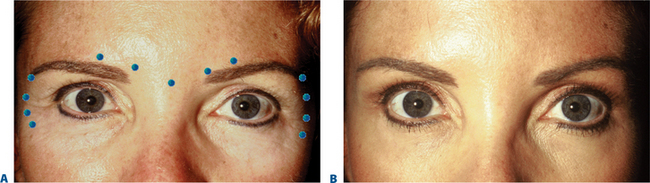
As previously mentioned, treating glabellar rhytides can also result in a pleasing brow lift. Adept clinicians can now predictably produce elevations in the medial, central, and temporal eyebrow. Varying treatments to the brow depressors have been shown to be effective in elevating the eyebrow through a host of techniques. Isolating treatment to the procerus, depressor supra-cilii, and lateral orbital orbicularis oculi muscle alone will elevate the brow but preserve its natural arc. Injecting 7 to 10 U BTX-A in the procerus at the midline, followed by one injection on each side (5 U) into the superolateral eyebrow at the temporal fusion line21 has been shown to be effective. This technique is especially useful in those individuals who exhibit brow ptosis and whose vertical glabellar frown lines are less of a concern (Fig. 24-18). This dramatically reduces the possibility of further brow depression (with any diffusion to the adjacent frontalis). By ignoring the variations in eyebrow shape presentation and the potential effects of treating the brow depressors in isolation, we fall short of delivering the optimum aesthetics (Fig. 24-19). Other techniques described demonstrate isolated injection of the lateral brow depressors13,14 by injection of 7–10 U into the superolateral orbicularis oculi at three sites below the lateral third of the brow, superior and lateral to the orbital rim, and produced significantly variable mid-pupillary and lateral brow elevations ranging from 1 to nearly 5 mm.13,14 The cause for such variability, while at first appearing confusing, might be more explainable than previously thought. Such variability has also been shown with surgical brow lifts, whereby the identical technique performed on various individuals can produce dramatically different results. The explanation most likely lies in the fact that precise application to the brow depressors can cause their dense chemo-denervation. The ‘lift’ ultimately will also depend on increased tone in frontalis.15 Significant brow elevation will be achieved after treatment to the brow depressors if the technique is precise. It is important to avoid injections ‘too high’ that may produce diffusion to the lateral frontalis (Fig. 24-20).


The potential effects and the ability to manipulate brow shape was a prelude to the recognition of the use of BTX for both the eradication of facial lines and as an agent for facial reshaping.4
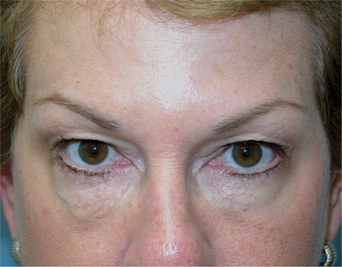
Some patients experience eyebrow asymmetry, for which BTX-A has also been beneficial. There are many causes of eyebrow asymmetry, including facial nerve trauma following surgical brow lift or other surgically induced facial paralysis, ipsilateral eyelid ptosis, and asymmetric non-pathologic facial expression.9 BTX-A injections into the brow depressors on the lower brow side can reset the balance (Fig. 24-11). Extreme care must be taken when treating non-pathologic facial asymmetry, both for the treatment of rhytids and brow position. Patients may look aesthetically improved in repose, but they might appear unusual with even casual animation when mobility (i.e. of the forehead) is only seen on the untreated side (Fig. 24-21).
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Evaluation of the Cosmetic Oculoplastic Surgery Patient
Evaluation of the Cosmetic Oculoplastic Surgery Patient
 Brow Lift Techniques
Brow Lift Techniques
 Treatment of Lower Eyelid Dermatochalasis, Herniated Orbital Fat, and Hypertrophic Orbicularis Muscle
Treatment of Lower Eyelid Dermatochalasis, Herniated Orbital Fat, and Hypertrophic Orbicularis Muscle
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Injectable Agents for Dermal Soft-Tissue Augmentation of the Face: Options and Decision Making
Injectable Agents for Dermal Soft-Tissue Augmentation of the Face: Options and Decision Making
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


