Exosomes, nanoscale extracellular vesicles, facilitate intercellular communication by delivering bioactive molecules such as proteins, lipids, and nucleic acids to target cells. Their therapeutic potential has gained significant attention in aesthetic and regenerative medicine for applications like wound healing, skin rejuvenation, pigmentation control, and hair growth. Studies reveal their ability to promote collagen synthesis, reduce inflammation, and regulate melanogenesis leading to improved skin repair and antiaging outcomes. Although promising preclinical and early clinical results highlight their efficacy, challenges in standardization, isolation methods, and comprehensive human trials remain hurdles in translating exosome-based therapies into widespread clinical practices.
Key points
- •
Exosomes, small extracellular vesicles, show potential in aesthetic medicine due to their role in cell communication and regeneration.
- •
The source of exosomes (eg, stem cells, blood, and adipose tissue) impacts therapeutic potential and safety.
- •
Current challenges include standardized exosome production, purity, and regulatory hurdles for clinical use.
- •
Despite promising preclinical results, there is need for rigorous clinical trials to confirm efficacy and safety.
- •
Food and Drug Administration (FDA) approval remains a major barrier, as exosome-based therapies currently lack regulatory clarity.
| AA | alopecia areata |
| ADSC-Exos | adipose stem cell-derived exosomes |
| AGA | androgenetic alopecia |
| DPC-Exos | DPC-derived exosomes |
| DPCs | dermal papilla cells |
| ESCRT | endosomal sorting complexes required for transport |
| EVs | extracellular vesicles |
| HACS | human adipose tissue stem cell-derived exosome solution |
| HPE | human platelet extract |
| IL | interleukin |
| MITF | microphthalmia-associated transcription factor |
| MMP | matrix metalloproteinases |
| MSCs | mesenchymal stem cells |
| MVBs | multivesicular bodies |
| PI3K/AKT | phosphatidylinositol 3-kinase/protein kinase B |
| PRP | platelet-rich plasma |
| TGF-β1 | transforming growth factor beta-1 |
| TNF-α | tumor necrosis factor alpha |
| TYR | tyrosinase |
| UCB-MSCs | umbilical cord blood mesenchymal stem cells |
Introduction
Exosomes are nanoscale, endosomal extracellular vesicles (EVs) known for their role in facilitating intercellular communication. EVs are broadly classified into 3 main categories: exosomes (30–150 nm), microvesicles (100–1000 nm), and apoptotic bodies (50–5000 nm) ( Fig. 1 ) [ ]. These vesicles serve as carriers for a wide array of lipids, proteins, and nucleic acids, enabling the precise delivery of biological signals to recipient cells. Exosomes have drawn the greatest interest among EVs due to their small size and biocompatibility, elevating their potential as therapeutic agents.
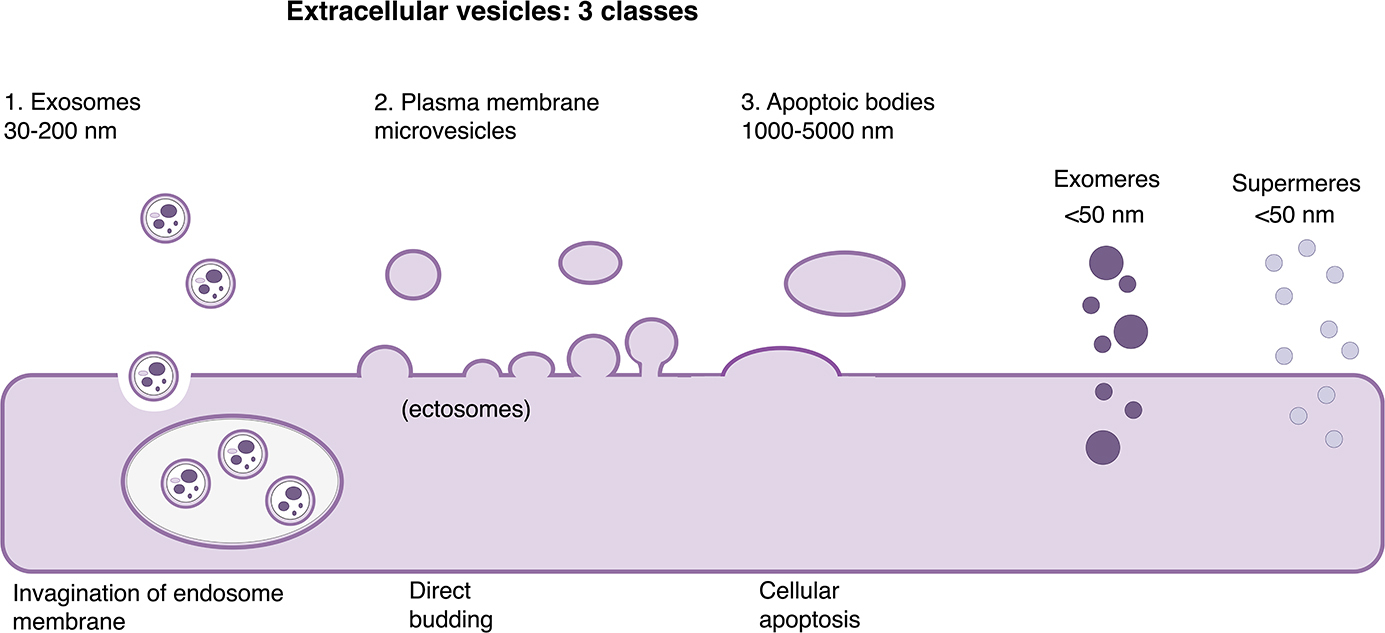
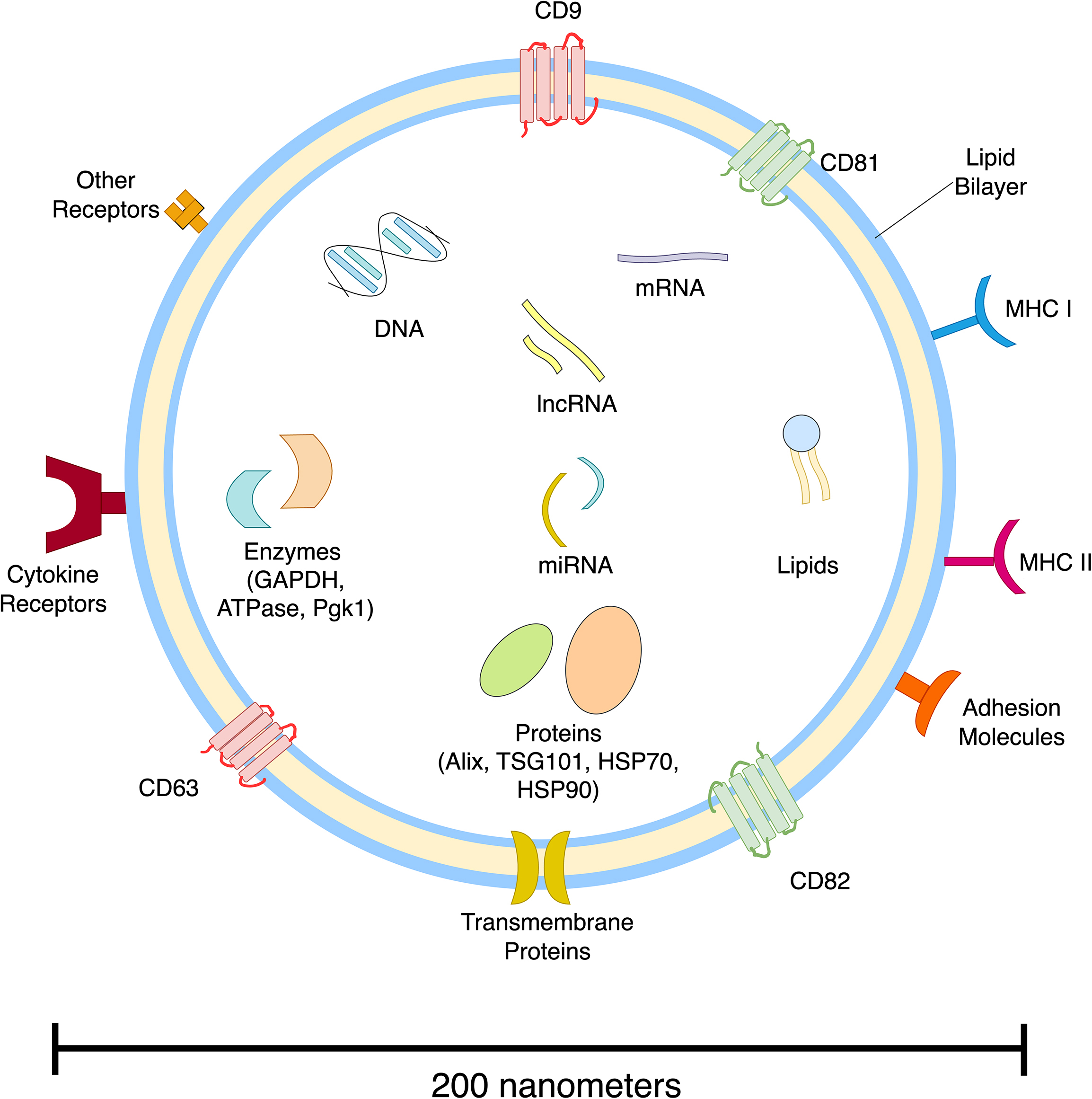
The formation of exosomes begins with the invagination of the plasma membrane, resulting in the development of early endosomes that mature into multivesicular bodies (MVBs). These MVBs release exosomes into the extracellular space through fusion with the plasma membrane. Encased in a protective lipid bilayer, exosomes transport a specialized cargo of proteins and nucleic acids that have been recognized to be reflective of their cell of origin ( Fig. 2 ). Moreover, MVB and exosome formation and release are primarily regulated through the endosomal sorting complexes required for transport (ESCRT) pathway, although ESCRT-independent pathways have also been proposed [ ]. Therefore, ESCRT pathway proteins such as Alix, TSG101, HSC70, and HSP90β are expected to be found in exosomes regardless of their origin cell [ ].
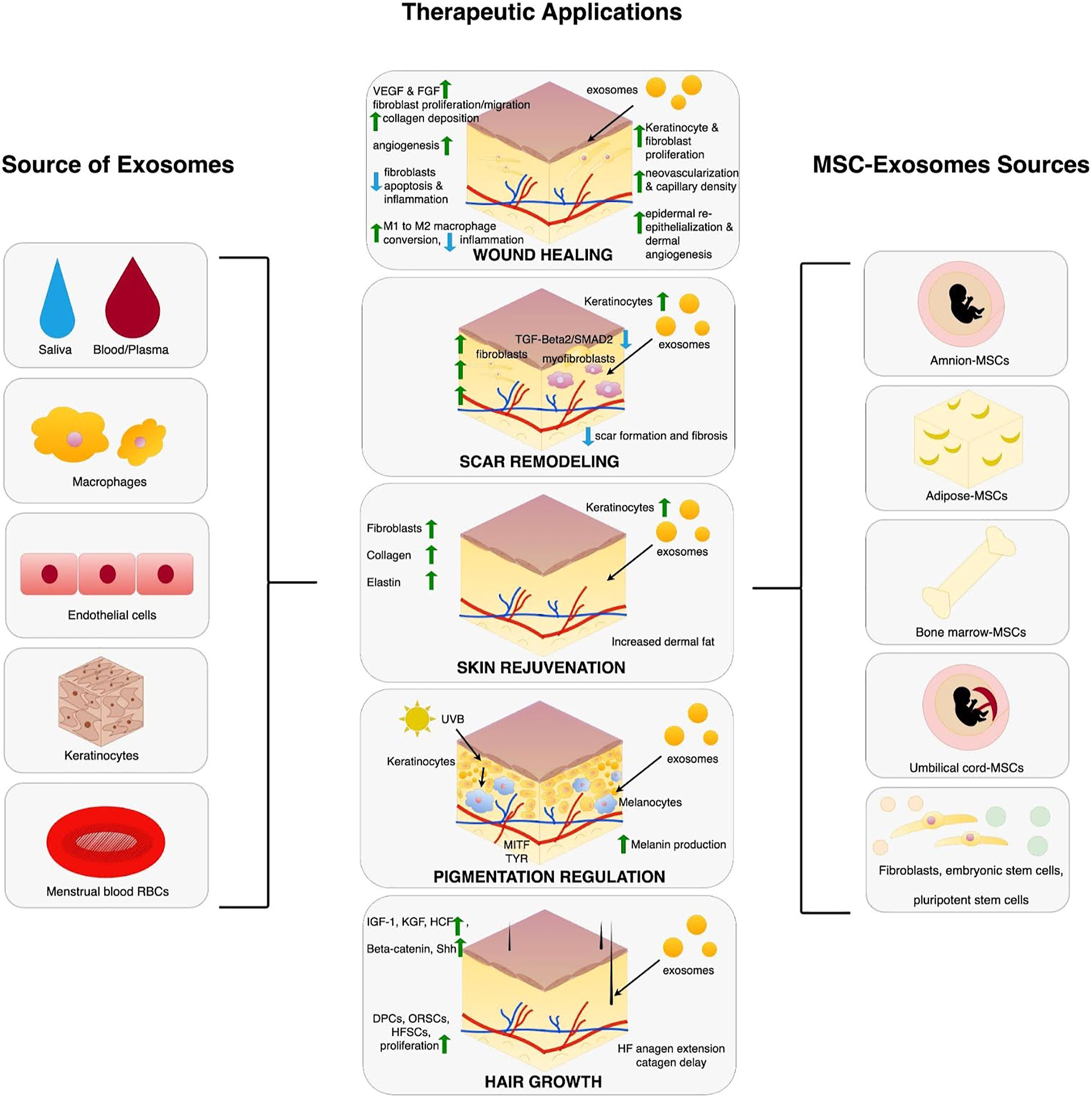
The biological function of exosomes is closely tied to their cellular source and determined by their cargo composition and downstream effects. Exosomes derived from mesenchymal stem cells (MSCs), keratinocytes, immune cells, endothelial cells, and platelets have distinct biochemical signatures and applications. For example, MSC-derived exosomes from sources such as adipose tissue, bone marrow, and umbilical cord are used to facilitate wound healing. Meanwhile, exosomes originating from endothelial cells are typically involved in angiogenesis signaling [ ].
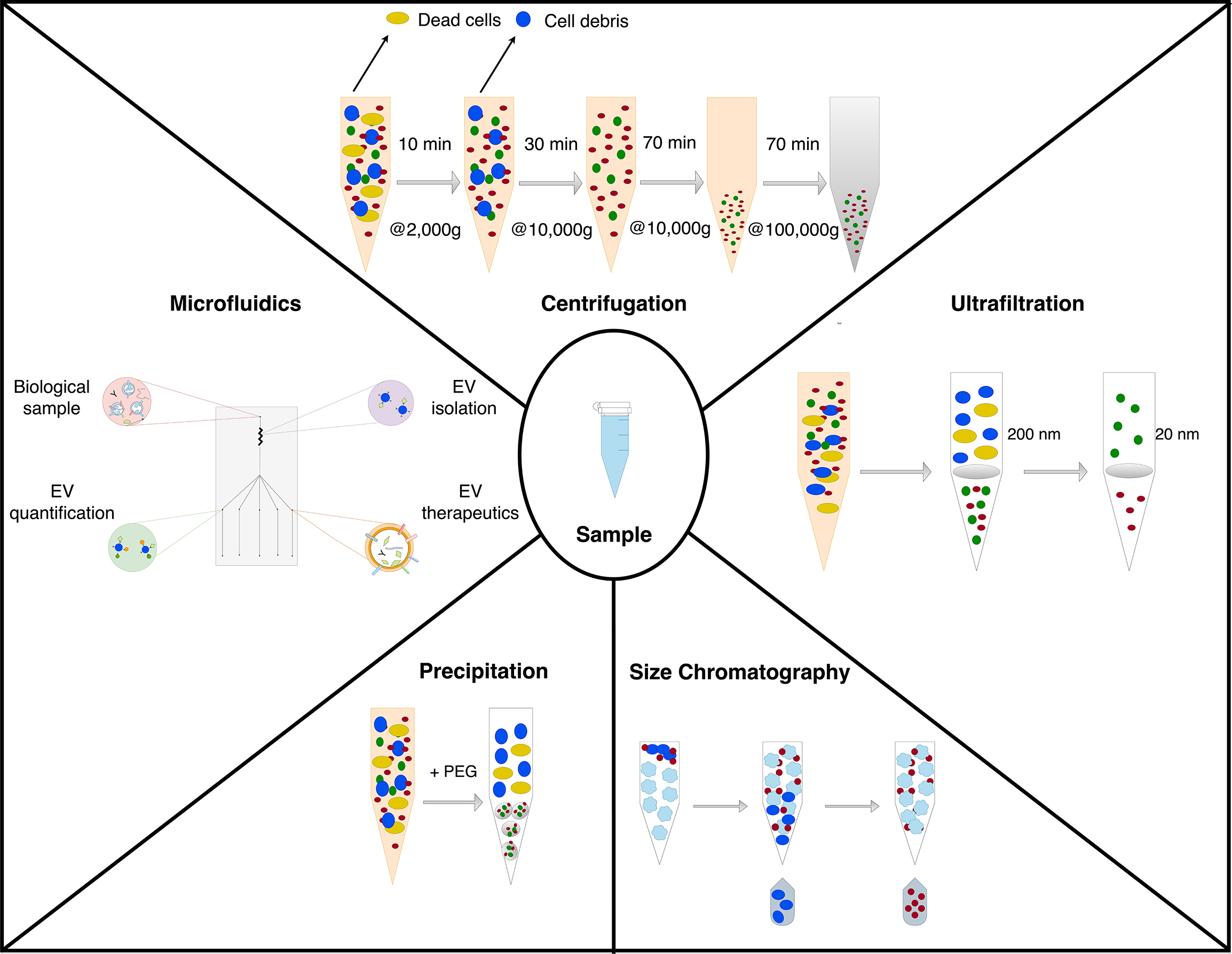
The process of isolating and purifying exosomes remains a technical challenge due to the heterogeneity of the exosome source. Several techniques are available for exosome isolation, including ultracentrifugation, ultrafiltration, polymer precipitation, and microfluidics-based methods ( Fig. 3 ). Among these, ultracentrifugation is the most widely used approach as it separates exosomes based on size and density [ ]. However, this method is time-consuming, costly, and may compromise the structural integrity of the vesicles. The choice of isolation technique must be tailored to the source of exosomes to ensure optimal recovery and preservation of functionality.
Despite these challenges, exosomes have emerged as valuable tools in therapeutic research and clinical applications. There is evidence that MSC-derived exosomes exhibit cardioprotective effects by improving cardiac function and lowering oxidative stress in myocardial ischemia-reperfusion models [ ]. Similarly, exosomes from macrophages can enhance immune responses by presenting MHC class II molecules to activate antigen-specific T cells, currently evaluated for applications in infectious diseases such as tuberculosis [ ].
The potential of exosomes in dermatology and in aesthetic medicine is only beginning to be explored. Emerging evidence highlights their role in key areas such as wound healing, skin rejuvenation, pigmentation modulation, and hair growth ( Fig. 4 ). A critical evaluation of these applications centers on the underlying mechanisms of exosome function and reported outcomes. Through their ability to mediate cellular communication and deliver targeted signals, exosomes hold the potential for many aesthetic therapeutic strategies. The current published data may have inherent biases favoring positive outcomes, emphasizing the need for more robust and substantiated clinical evidence to validate their efficacy and safety.
Clinical applications
Healing and Scar Remodeling
Wound healing is a dynamic and complex biological process involving multiple overlapping phases: inflammation, proliferation, and remodeling. Effective repair requires the coordination of diverse cell types, including keratinocytes, fibroblasts, inflammatory and endothelial cells, which collectively contribute to re-epithelialization, angiogenesis, and remodeling. Exosomes have emerged as promising therapeutic agents in wound healing due to their applicability in mediating intercellular communication.
In vitro and animal studies
Over 50 studies have explored exosome roles in dermal wound healing in rodent models [ ]. The primary source of exosomes in these studies were mesenchymal stem cells (40%) or umbilical stem cells (10%), but other sources include human platelet-rich plasma (PRP), human umbilical vein endothelial cells, fibroblasts, keratinocytes, and macrophages. The most common isolation technique reported was ultracentrifugation and the most common method of administration was subcutaneous injection. Despite the heterogeneity of molecular cargo across studies, exosomes were found to have therapeutic properties and aid in cutaneous wound healing, regardless of the model, mode of administration, exosome concentration, the number of administrations, or the source of exosomes. Exosome cargo varied with most published studies focusing on microRNA-21 (miR-21). The proposed mechanisms by which miR-21 influences wound healing is by stimulating angiogenesis and activating the phosphatidylinositol 3-kinase/protein kinase B (PI3K/AKT) pathway. Overall, exosome administration has shown to significantly improve wound closure in 81% of mice studies, enhance vascularity in 50%, and promote collagen deposition and wound-bed viability. Other reported outcomes included increased fibroblast proliferation, improved collagen maturation, and reduced scarring [ ]. Similarly, in diabetic wound healing studies, stem cell derived exosomes are primarily used, but sources such as menstrual blood and bovine milk have been studied [ ]. Published evidence indicates that exosome therapy can improve diabetic wound healing rates, neovascular density, re-epithelialization, collagen deposition, and scar width. Additionally, analyses of inflammatory markers have demonstrated decreased levels of interleukin (IL)-6, IL-1β, and tumor necrosis factor alpha (TNF-α) [ ].
In scar remodeling, adipose stem cell-derived exosomes (ADSC-Exos) have demonstrated notable efficacy in the treatment of keloids by enhancing mitochondrial autophagy via modulation of the phosphoinositide 3-kinase/protein kinase B/mechanistic target of rapamycin (PI3K/AKT/mTOR) pathway [ ]. ADSC-Exos with noncoding ribonucleic acid (RNAs), particularly miR-194, significantly reduced hypertrophic scarring by downregulating transforming growth factor beta-1 (TGF-β1) expression, thereby affecting aberrant fibroblast proliferation and collagen synthesis [ ].
Clinical studies
ADSC-Exos have been studied as adjuvant therapy for atrophic acne scars treated with fractional CO 2 laser. In a randomized, split-face study including 25 patients the ADSC-Exos treated side reported better scar reduction compared to untreated controls (32.5% vs 19.9%), reduced posttreatment erythema, and supposedly shorter recovery times (4.1 days vs 4.3 days). There were no exosome specific adverse effects reported in this series [ ].
In a double-blind, placebo-controlled clinical study assessed the safety and potential therapeutic effects of platelet-derived exosomes in healthy participants (n = 11). Participants were subjected to wounds from a 4 mm punch biopsy on inner arms, with 1 site treated with exosomes (100 μg) and the other with isotonic solution. Both the treatment and placebo groups achieved complete wound closure within an average of 22.8 ± 8.7 days, and all wounds were fully healed by day 30. No serious adverse events were noted [ ].
A phase II clinical trial consisting of 32 participants investigated the topical application of 10% secretome gel derived from human umbilical cord mesenchymal stem cells(UCB-MSCs) for treating chronic ulcers caused by diabetes (5 participants) and leprosy (27 participants). The study demonstrated significant reductions in wound length (from 2.41 cm to 1.65 cm), width (from 1.83 cm to 1.19 cm), and area (from 6.69 cm 2 to 4.00 cm 2 ) 1 month after treatment with no adverse effects reported [ ].
Skin Rejuvenation
Skin aging is a multifaceted process driven by both intrinsic factors, such as genetics and metabolic processes, and extrinsic factors, including ultraviolet radiation. These factors collectively cause structural and functional changes in the skin, particularly within the extracellular matrix. Photodamage plays a significant role in skin aging by fragmenting collagen, reducing its production, and accumulating abnormal elastin and degraded collagen, which contribute to wrinkles, loss of firmness, and uneven skin texture. Exosomes are increasingly emphasized as promising therapeutic agents to mitigate these effects by promoting collagen synthesis and reducing matrix degradation.
In vitro and animal studies
In vitro studies on human dermal fibroblasts show that exosomes from human umbilical cord blood mesenchymal stem cells (UCB-MSCs) can induce fibroblast migration and increase expression of collagen I, fibronectin and elastin, while reducing matrix metalloproteinases (MMP)-1 levels [ ]. Similarly, in animal studies, ADSC-Exos were shown to increase type I collagen and decrease type III collagen and MMP 1/3 [ ]. In animal models of photoaging, subcutaneous injection of ADSC-Exos preserved the thickness of the epidermis and dermis following ultraviolet B (UVB)-radiation [ ]. Exosomes derived from three-dimensional (3D) spheroid-cultured human fibroblasts demonstrated superior efficacy to monolayer fibroblast and MSC demonstrating more collagen synthesis, reduced inflammation, and better mitigation from UVB-photoaging in mice [ ]. The mechanism involved downregulation of TNF-α and upregulation of TGF-β, which enhanced type I procollagen production and reduced MMP-1 expression. Exosomes derived from embryonic stem cells, such as those containing mmu-miR-291a-3p, were shown to inhibit cellular senescence in human fibroblasts by targeting the TGF-β pathway, restoring telomere length, and reducing deoxyribonucleic acid (DNA) damage [ ].
Clinical studies
There are several studies demonstrating some evidence of exosomes improving aging features. In a 12-week randomized, split-face study with 28 participants (20 F, 8 M; skin type III-IV; age 54.0 ± 7.8 (43–66) years), human adipose tissue stem cell-derived exosome solution (HACS) applied before microneedling (1 mm) significantly reduced wrinkles (12.4% vs 6.6%, P ≤.031), increased elasticity (11.3% vs a 3.3%, P =.002), increased hydration (6.5% vs 4.5%, P =.037), and reduced melanin index (9.9% vs 1.0%, P =.044) compared to control. Histopathological findings revealed enhanced collagen and elastic fiber density, further demonstrating the superior efficacy of the HACS treatment [ ].
In a randomized, double-blind, placebo-controlled study with 40 patients (30 F, 10 M; age 32–76 years; 22 white and 18 nonwhite), a topically applied human placental MSC exosomes group (n = 20) showed significant improvements in skin tone, clarity, vascularity, and wrinkle reduction ( P <.0001) with 75% reporting being extremely satisfied by day 120, compared to 0% in the control group, and no adverse reactions reported [ ].
Human platelet extract (HPE) is an allogeneic exosome product derived from leukocyte-reduced apheresed platelet. A clinical trial on the safety and tolerability of HPE with 56 participants (48 F 8 M; age 54 ± 11 (40–80) years; skin types I-IV) with mild to moderate global face wrinkles demonstrated statistically significant improvement in overall skin health score after 6-week use. There was a notable reduction in erythema area by −2.39 ( P =.005), brown spot fractional area by −0.0161 ( P ≤.0001), and wrinkle fractional area across facial regions by 0.01 to 0.04 ( P ≤.0023). Luminosity scores increased by 5.42 ( P ≤.0001), and color evenness improved by 0.071 ( P ≤.0001) Skin texture, radiance, and firmness improved on average 0.3, 0.4, and 0.1 points, respectively There was no visible improvement in skin sagginess [ ].
Pigmentation Control
Exosomes have the potential to modulate pigmentation by regulating melanin synthesis and enhancing melanosome degradation, offering therapeutic promise for conditions like melasma and hyperpigmentation.
In vitro and animal studies
Keratinocyte-derived exosomes with miR-675 and miR-330-5p can inhibit melanogenesis by directly targeting microphthalmia-associated transcription factor (MITF). MITF is a pivotal transcription factor that governs the expression of tyrosinase (TYR) and other proteins essential for melanin production [ ]. Similar mechanism of MITF downregulation has been described with miR-181a-5p Exo from human amniotic MSC [ ]. Exosomes containing miR-199a can increase melanosome degradation through autophagy activation [ ]. Interestingly, exosomes derived from hypertrophic scar fibroblasts significantly reduced the mRNA and protein expression of pigmentation-related factors, including paired box-3 (Pax3), sex-determining region Y-related high mobility group-box-10 (Sox10), MITF, TYR, and TYR-related proteins [ ].
Clinical studies
Clinical studies evaluating the efficacy of exosomes in pigmentation control are limited. One open-label study including 12 female participants (46.64 ± 13.05 year old) with Fitzpatrick types II-IV with moderate-to-severe facial hyperpigmentation evaluated the efficacy of rose stem-cell-derived exosomes combined with microneedling. By week 12, participants exhibited a 13% reduction in superficial pigmentation, a 16% reduction in deep pigmentation, a 7.34% reduction in redness, and a 6.3% improvement in skin quality, with no major adverse events reported. Psychometric scores for life quality also significantly improved [ ].
Hair Growth
The use of exosomes in hair growth regulation and as therapy for alopecia is still in nascent stages.
In vitro and animal studies
Most current evidence derived from in vitro and animal studies centers on regulation of the hair follicle growth cycle by dermal papilla cells (DPCs) [ ]. DPC-derived exosomes (DPC-Exos) have shown the most promise primarily by enhancing Wnt/β-catenin signaling, a critical pathway for hair growth and regeneration. In animal studies, DPC-Exos can stimulate the early onset of anagen phase, delay the catagen, and upregulate key signaling molecules such as sonic hedgehog, keratinocyte growth factors, and β-catenin [ ].
ADSC-Exos also demonstrate potential in promoting hair growth by mitigating dihydrotestosterone effects, primarily by downregulating TGF-β1 signaling and through targeting small mother against decapentaplegic family member 3 (SMAD3) (miR-122-5p) [ ]. When compared to PRP exosomes, ADSC-Exos are found to support hair growth by increasing proliferation of human DPCs, dermal thickness, and hair bulb size [ ].
Clinical studies
Exosome-based therapies are a promising avenue for treating androgenetic alopecia (AGA), alopecia areata (AA), and hair disorders. The strength of clinical evidence remains limited as most trials are industry-sponsored, lack transparency and scientific rigor. Many reports combine exosome injections with adjunctive hair procedures such as microneedling and lasers, both of which independently benefit hair growth, complicating the interpretation of exosome-specific effects.
In AGA, foreskin-derived MSC exosomes scalp injections of 30 AGA patients (30 M; age 22–65 years; hair loss III-VI, Norwood-Hamilton). After 12 weeks, a statistically significant increase in hair density was observed, with no adverse events reported [ ]. Similarly, ADSC-Exos delivered via microneedling to 39 patients with male and female pattern hair loss showed marked improvements in hair density and thickness after 12 weekly sessions [ ]. Aside from microneedling-related discomfort, no exosome-related adverse effects were noted. Multiple sessions of ADSC-Exos scalp therapy with microneedling (n = 30; AGA; 16 F 14 M; age 47 ± 7.58) significantly increased hair density, with mild, temporary scalp redness and tingling [ ]. Recent comparative study positions exosomes superiorly to PRP treatments, with better outcomes in hair regrowth after fewer sessions and maintained results for up to 28 months, with no serious adverse events in either group.
Exosome-based therapies have also been trialed for AA. Rose stem cell-derived exosomes applied through electroporation in one AA patient improved hair density and reduced hair loss after 12 sessions without adverse events. A combination of rose stem cell exosomes with fractional picosecond laser treatments in another patient with AA and poliosis circumscripta, yielded additional benefits, with restored hair growth and pigmentation in affected areas [ ].
MSC exosomes have shown potential in treating acquired trichorrhexis nodosa, a hair shaft disorder characterized by fragility and breakage. In a case series involving 3 patients, monthly scalp injections of MSC exosomes led to improvement in hair density, length, pigmentation, and cuticle recovery. These results were sustained at 1-year follow-up, as confirmed by photographic documentation, dermoscopy, and scanning electron microscopy [ ].
Limitations
Exosome-based therapies hold significant promise in aesthetic and regenerative medicine; however, multiple barriers exist that must be addressed before their widespread use and commercialization. The primary limitation lies in the lack of standardization in exosome production, which affects the consistency and reliability of therapeutic outcomes. Variability in source material, isolation techniques, and purification methods introduces biological heterogeneity, leading to inconsistencies in exosome yield, content, and quality. Additionally, storage conditions and the absence of regulatory oversight in exosome preparation contribute to uncertainties regarding the purity and functional integrity of marketed exosome products.
Another major concern is the limited clinical evidence supporting exosome efficacy and safety in humans. Exosomes present unique theoretic risks, including their potential to carry oncogenic material from donor cells, modulate immune responses or encapsulate pathogens such as prions and viruses. Achieving targeted delivery to specific tissues remains a technical hurdle, as exosomes can circulate systemically and interact with off-target cells, potentially leading to unintended organ effects. Questions also remain about the duration of exosome activity in the body, with concerns regarding implications for prolonged or delayed effects.
While preclinical studies and early-phase trials report promising results, clinical data remain sparse, and lack robust design, appropriate controls, standardized dosages, and long-term follow-ups. The safety profile of exosomes in aesthetic use is not fully understood. While topical exosome applications are generally considered safe, adverse events such as granulomas, necrosis, and anaphylaxis have been reported in cases with adjunct skin barrier disruption [ , ]. Additionally, the FDA has warned the use of exosome products following a report of five patients in Nebraska experiencing serious adverse events including bacteremia after the use of exosome product derived from C-sectioned placentas [ ].
Currently, the only one FDA-approved stem cell-based product contains hematopoietic progenitor cells derived from cord blood, indicated for limited use in patients with hematologic disorders or malignancies. No exosome-based products have received FDA approval yet. The FDA has addressed misleading claims by some clinics suggesting that these products are not subject to regulatory provisions for drugs and biological products, stating such claims are “simply untrue.” However, stem cell-derived therapies can be offered in clinical trials under an Investigational New Drug application—a clinical investigation plan reviewed and approved by the FDA. Addressing limitations will require well-designed clinical trials, stringent manufacturing standards, and comprehensive regulatory frameworks to ensure the safety, efficacy, and scalability of exosome-based therapies.
Summary
Exosome-based therapies represent a potentially transformative innovation in aesthetic and regenerative medicine, with applications spanning wound healing, skin rejuvenation, pigmentation regulation, and hair growth. Evidence from preclinical and clinical studies highlights their capacity to facilitate cellular communication, collagen synthesis, regulate melanogenesis, and modulate inflammation, yielding encouraging outcomes. However, challenges remain, particularly regarding standardization and variability in isolation techniques, underscoring the need for rigorous investigation to ensure optimal efficacy and safety. Advancing this field will require greater transparency about exosome composition and the role of adjunctive therapies. While the promise of exosome-based treatments is significant, further large-scale, independent, and well-designed studies are essential to validate their clinical effectiveness and elucidate mechanisms of action.
Clinics care points
- •
The support for the use of exosomes in human cutaneous applications is limited.
- •
There is evidence for application of exosomes in wound healing and scar remodeling from animal models, and the limited human trials support potential for enhanced recovery time and scar remodeling.
- •
In esthetics, exosomes have been shown to enhance outcomes including wrinkle reduction, hydration, hyperpigmentation control, and hair growth, usually when combined with adjunct therapies, such as microneedling.
- •
Be cautious when selecting and using exosome products, as variability in source and preparation methods can lead to inconsistent formulations. Always prioritize products that meet stringent quality and safety standards.
- •
All patients considering exosome-based treatments should be thoroughly educated about associated risks, potential side effects, and the current lack of FDA approval for these therapies.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


