The prevalence and emotional impact of acne scarring are underestimated by the medical community. Dermatology providers should be able to evaluate the acne scar patient and discuss treatment options. Important aspects of the patient history include current treatments, prior acne scar procedures, and the patient’s goals for treatment. During the physical examination, the scars are assessed and classified by scar morphology and overall severity of scarring. Finally, a treatment plan is developed in which the most appropriate procedures are matched with the scars that will work the best. Helping the patient understand likely expectations for improvement will increase overall satisfaction.
Key points
- •
Dermatology providers should be capable of evaluating patients with acne scars and have a discussion about treatment options.
- •
During the history and physical examination, the morphology and severity of acne scars are assessed, as are the patient’s goals for treatment.
- •
A treatment plan that sets appropriate expectations and includes the most effective treatments by scar morphology and severity will maximize patient satisfaction.
Introduction
Acne scarring is an unfortunate long-term complication that can affect up to 95% of patients who have acne vulgaris. The prevalence of acne scarring in the general population is estimated to be 1% to 11%. Dermatologists should not underestimate the importance of addressing the topic of acne scars with patients. Having acne scars can be emotionally distressing to patients and can affect all aspects of their lives. Indeed, acne scars have been linked to depression, suicide, anxiety, poor self-esteem, social impairment, lowered academic performance, and unemployment. Because of the profound effect the scars can have on a patient’s quality of life, dermatology providers should take the time and develop the skills to effectively evaluate acne scars and counsel patients regarding treatment.
Although scarring can occur with any type of acne, early treatment of inflammatory and nodulocystic acne is the most important way to prevent acne scars. Scars that develop during a few brief years of adolescent acne persist through the rest of life, and in some cases can worsen with normal aging or photodamage. Once the scars develop, treating them can be difficult, expensive, time consuming, and often incomplete. This disease is truly one in which “an ounce of prevention is worth a pound of cure.”
This report covers the evaluation of the acne scar patient and the initial discussion in which a treatment plan is established and expectations are set. A comprehensive review of each acne scar procedure is beyond the scope of this work. As with any consultations, a pertinent history and physical examination is performed, followed by a thoughtful assessment and the development of a personalized treatment plan that appropriately addresses the patient’s goals for improvement. The discussion is limited to the evaluation and management of atrophic acne scars. Several other works have expertly discussed the management of keloidal acne scarring.
Introduction
Acne scarring is an unfortunate long-term complication that can affect up to 95% of patients who have acne vulgaris. The prevalence of acne scarring in the general population is estimated to be 1% to 11%. Dermatologists should not underestimate the importance of addressing the topic of acne scars with patients. Having acne scars can be emotionally distressing to patients and can affect all aspects of their lives. Indeed, acne scars have been linked to depression, suicide, anxiety, poor self-esteem, social impairment, lowered academic performance, and unemployment. Because of the profound effect the scars can have on a patient’s quality of life, dermatology providers should take the time and develop the skills to effectively evaluate acne scars and counsel patients regarding treatment.
Although scarring can occur with any type of acne, early treatment of inflammatory and nodulocystic acne is the most important way to prevent acne scars. Scars that develop during a few brief years of adolescent acne persist through the rest of life, and in some cases can worsen with normal aging or photodamage. Once the scars develop, treating them can be difficult, expensive, time consuming, and often incomplete. This disease is truly one in which “an ounce of prevention is worth a pound of cure.”
This report covers the evaluation of the acne scar patient and the initial discussion in which a treatment plan is established and expectations are set. A comprehensive review of each acne scar procedure is beyond the scope of this work. As with any consultations, a pertinent history and physical examination is performed, followed by a thoughtful assessment and the development of a personalized treatment plan that appropriately addresses the patient’s goals for improvement. The discussion is limited to the evaluation and management of atrophic acne scars. Several other works have expertly discussed the management of keloidal acne scarring.
History
During the initial visit, a history is taken. Important parts of the history are listed in Box 1 . First, an assessment of the status of the patient’s current acne is essential. Active acne is best brought under control before any acne scar procedures are initiated. If acne has cleared recently, perceived scars may only be red or dark purple macular dyspigmentation that often clears on its own without any intervention. Current and past treatment of acne is assessed. Most importantly, recent isotretinoin use should be noted, as this may necessitate a delay in some resurfacing procedures.
Current acne assessment
Is your acne under control?
How long has it been clear?
What treatments are you currently on?
Patient-specific questions
What bothers you the most about your skin?
Which scars or areas of your face concern you the most?
How are the acne scars affecting your life?
Questions that may affect treatment options
Have any prior procedures been performed to treat the scars? If so assess:
Number of sessions, associated downtime, efficacy, problems healing
What are your goals for treatment?
Was Isotretinoin used to clear the acne? When was your last dose?
Have you had any darkening of your skin from acne, surgery, or injury?
Do you have any painful, thick, or itchy scars on your body?
Next, the patient’s specific concerns and goals should be assessed. General questions such as “What bothers you about your skin?” or “what areas or scars you are most interested in improving?” are open-ended questions that allow the patient to express his or her desires and preferences, which may guide treatment planning. Not uncommonly, a patient may be concerned about a specific scar or area of scarring that does not appear to be the most obvious to the physician. Targeting certain scars that are most concerning to the patient may increase the chance for successful treatment and patient satisfaction.
Along with addressing active acne and assessing the patient’s goals, personal and family skin history should be addressed. Are there other family members with acne scars, such as a parent or sibling? A question about history of hyperpigmentation after prior acne, inflammation, injury, or surgery will help the physician evaluate the risk of postinflammatory hyperpigmentation from energy-based or surgical procedures. Any prior procedures for acne scars should be noted, including the type of procedure, associated downtime, number of sessions, any abnormal healing, and degree of improvement.
Finally, an assessment of the patient’s specific goals and expectations is taken. This assessment includes the ability to tolerate pain, tolerability of downtime, and any time constraints, such as work or travel. This assessment is an important time for the provider to assess any unrealistic expectations or signs of body dysmorphic disorder, which would be contraindications to initiating treatment.
Physical examination
The examination of the acne scar patient includes visual inspection under appropriate lighting, active palpation of the skin, and classification of types and severity of scars. Directional or overhead lighting often helps reveal the textural irregularities. A hand-held mirror allows the patient to point out specific concerns and feel like they are completely understood. Pearls for the physician examination are listed in Box 2 .
- •
Evaluate for active acne.
- •
Use directional lighting shined tangentially on the skin to highlight atrophy/textural change.
- •
Have a mirror for the patient to point out lesions.
- •
Define types of scars (ice pick, rolling, boxcar, severely atrophic/sclerotic).
- •
Assess color (hypopigmentation, hyperpigmentation, purple/red discoloration).
- •
Assess depth and width of lesions.
- •
Stretch skin to see if scars disappear.
- •
Palpate for underlying fibrosis.
- •
Evaluate skin type (types III–V have increased risk of PIH with most procedures).
When visually inspecting scars, the physician should look at the scar morphology. Important scar characteristics are the depth, width, margin characteristics (sharply defined, vertical shoulder vs a gently sloping shoulder), and quality of skin at the base. Scars with normal skin at the base are amenable to more treatment options, whereas scars with hypopigmented or sclerotic skin require excisional or aggressive resurfacing procedures for improvement. Total number of scars and distribution may affect treatment plan decisions. For example, having less than 5 deep ice pick acne scars might allow a patient to be treated by a single session of punch grafting or punch excision. Alternatively, a patient with more than 100 similar lesions might be approached with a series of resurfacing procedures, as performing the required number of surgical procedures might be unfeasible because of time constraints and the densely packed nature of the lesions.
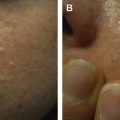
Multiple acne scar classification systems have been proposed. The simplest and arguably the most practical system divides atrophic acne scars into 3 types based on morphology: ice pick, rolling, and boxcar scars ( Fig. 1 ). Ice pick scars have a narrow diameter, sharply defined shoulders, and deep depth. Rolling scars have a gently sloping border and are wider than they are deep ( Fig. 2 ). Boxcar scars have sharp, vertical borders which drop down to a flat base and most closely resemble varicella scars. It is common for patients to have more than one type of scar. Another useful grading system proposed by Goodman and Baron uses a 4-point scale grading system to stratify severity of scarring ( Box 3 ).
Related posts:
 The Relationship of Proper Skin Cleansing to Pathophysiology, Clinical Benefits, and the Concomitant Use of Prescription Topical Therapies in Patients with Acne Vulgaris
Top Ten List of Clinical Pearls in the Treatment of Acne Vulgaris
Use of Oral Contraceptives for Management of Acne Vulgaris
The Relationship of Proper Skin Cleansing to Pathophysiology, Clinical Benefits, and the Concomitant Use of Prescription Topical Therapies in Patients with Acne Vulgaris
Top Ten List of Clinical Pearls in the Treatment of Acne Vulgaris
Use of Oral Contraceptives for Management of Acne Vulgaris
 Evaluation and Management of Refractory Acne Vulgaris in Adolescent and Adult Men
Physical Modalities (Devices) in the Management of Acne
Evaluation and Management of Refractory Acne Vulgaris in Adolescent and Adult Men
Physical Modalities (Devices) in the Management of Acne
 When Acne is Not Acne
When Acne is Not Acne
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


