Acne vulgaris alters the normal skin physiology, impairing stratum corneum and transepidermal water loss. A male’s normal skin physiologic state is different than a female’s and may have implications when choosing treatment when the skin is altered in a disease state. Transepidermal water loss, pH, and sebum production are different between the sexes. Several underlying conditions present in male acne patients at several ages that may require a more in-depth evaluation. As knowledge of the pathogenesis of acne expands, the differences in skin physiology between the sexes may alter the manner in which male patients with acne medications are approached.
Key points
- •
A male’s normal skin physiologic state is different than a female’s and may have implications when choosing treatment when the skin is altered in a disease state.
- •
Transepidermal water loss, pH, and sebum production are different between the sexes.
- •
Acne vulgaris alters the normal skin physiology, including impairment of the stratum corneum and transepidermal water loss.
- •
There are several underlying conditions presenting in male acne patients at several ages that may require a more in-depth evaluation.
Men are from Mars and women are from Venus , but is this true when treating male patients with acne? Several skin physiologic variances exist between the sexes and may lead physicians to approach their male acne patients differently. Several aspects, including transepidermal water loss (TEWL), pH, and sebum production, have all been demonstrated to be different between the sexes. Adolescent and adult men are also more likely to be affected by seborrheic dermatitis, which shares a similar inflammatory cascade to acne pathogenesis and which may have therapeutic implications for acne. Adolescent and adult men may also consume supplements that increase their insulin growth factor-1 and predispose them to developing more acne. There are also several underlying conditions presenting with acne in adolescent and adult men in several age groups that may require further investigation. As more is learned about skin physiology and the pathogenesis of acne, these few baseline skin physiologic differences may in fact change the approach to male patients with acne in the future.
TEWL has recently become an important concept in dermatology and when approaching patients with acne. According to Luebberding and colleagues, in examination of 300 healthy men and women, TEWL was found to be significantly lower in the male cohort than the water loss of women in the same age category until age 50. The implications of this finding are important in the treatment of acne in adolescent male patients. Yamamoto and colleagues demonstrated that patients with acne have impairment of the stratum corneum and TEWL. This impairment of the stratum corneum correlates with the burden of disease. If adolescent male patients begin with a baseline TEWL lower than adolescent female patients, and then develop moderate to severe acne that affects the normal baseline function of their stratum corneum, adolescent male patients in theory would deviate farther from their normal physiologic state and perhaps be more prone to adverse side effects of acne therapies that augment barrier function more than female patients. Harper demonstrated gender and age differences between male and female patients and found improved treatment success with clindamycin phosphate 1.2%/benzoyl peroxide 2.5% gel in young adolescent women and older adult men. The Harper study supports the differences outlined in the research of Luebberding and colleagues of gender variance based on age of male and female patients, demonstrating TEWL becomes more similar with age. Nearly all of the medications used in the dermatology armamentarium augment barrier function, including benzoyl peroxide, topical retinoids, and isotretinoin. However, if TEWL and stratum corneum function are maintained at near normal levels by the practitioner when treating male acne patients, medications that target key gender differences may improve outcomes in acne treatment. Preservation of TEWL and stratum corneum health is a target area for new therapeutic formulations in the future of acne treatment.
The pH of physiologically normal skin is 5.4. However, male patients have significantly lower pH values, less than 5.0, than female patients, which are higher than 5.0, regardless of age. Free fatty acids are elevated in male skin because of higher production of sebum, causing the pH to be different from female patients. Although the implications of pH in acne pathogenesis have not yet been elucidated, as more is learned, the pH difference may have implications when developing appropriate acne treatment formulations for proper delivery of topical medications between the sexes.
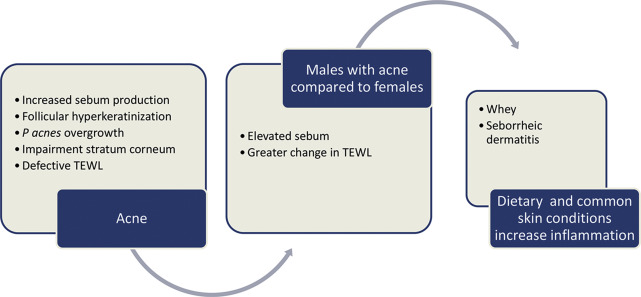
Sebum production is elevated in male patients in comparison with female patients. Even though elevated sebum production alone does not induce acne, alterations in sebum composition have been demonstrated to cause follicular hypercornification via stimulation of the innate immune system directly and indirectly. Sebum also promotes an anaerobic environment for Propionibacterium acnes to thrive. P acnes is able to drive inflammatory cytokines through toll-like receptors 2 and 4 (TLR); this is followed by elevated production of interleukin (IL)-1β, which induces IL-6, IL-8, and IL-12. Eventual stimulation of activator protein-1 causes activation of matrix metalloproteinases (MMPs) and theoretic increase for scar formation. Adolescent and adult men, in theory, are at increased risk of developing acne scarring based on elevated sebum production and upregulation of the inflammatory cascade compared with female acne patients ( Fig. 1 ). Therefore, topical and oral retinoids may be even more beneficial in male patients because of their direct effect on the sebaceous gland activity, leading to a greater degree of reduction in sebum and inhibition of inflammation and eventual MMPs that cause scar formation.
Seborrheic dermatitis is a chronic dermatitis that affects 5% of the population, with young men comprising a large proportion. The male population overrepresentation is thought to be from excessive sebum compared with other affected cohorts. In the past, seborrheic dermatitis was thought to be solely from overgrowth of Malassezia species that flourish in more oil-prone areas. Recent data have discovered dandruff sufferers actually have a mixed bacterial and fungal imbalance that predisposes them to this chronic issue. One of the implicated bacterial species is P acnes . Examination of the purposed inflammatory cascade of seborrheic dermatitis activates the innate immune stimulation by Malassezia restricta through the nodlike receptor 3 (NLRP3) on sebocytes that induce IL-1β. The nodlike receptors are a class of pattern-recognition receptors similar in function to TLR. P acnes has also been demonstrated to activate this cascade through NLRP3. P acnes –induced inflammation is reduced in NLRP3-deficient mice. Adolescent and adult men are more likely to suffer from seborrheic dermatitis, and this NLRP3 inflammatory cascade may be more amplified in adolescent and adult men also affected by acne because they share a similar pathway. Treatment of both the seborrheic dermatitis and the acne is an important therapeutic consideration to diminish overstimulation of this inflammatory cascade shared by these 2 micro-organisms. However, more controlled trials examining these cohorts are needed to solidify this association.
Finally, some food for thought in regard to diet and acne: whey. The whey protein supplement market has doubled since 2007 with annual sales of $396 million last year. As of 2012, 1 in 10 men were using sports supplements at least once a week. Whey protein, which has been linked to an increase in insulin growthlike factor-1, stimulates sterol response binding protein-1 that can stimulate sebaceous gland lipogenesis, comedogenesis, follicular inflammation, and androgenic stimulation (see Fig. 1 ). One case series noted improvement of acne severity with elimination of whey supplementation. However, more random controlled trials are required to prove the association with acne severity; however, it is a unique consideration regarding the male acne patient population.
There are several underlying conditions that may present in male patients with acne. Classical congenital adrenal hyperplasia is more commonly recognized in female patients because of noted virilization on examination. The patients also present with salt wasting soon after birth. However, there is a nonclassical form that presents later in life. Young men presenting with precocious puberty, increased axillary and pubic hair, enlarged penis, and acne before the age of 9, should trigger an evaluation for the nonclassical form of congenital adrenal hyperplasia. Hand radiographs for bone age is an appropriate screening tool. Laboratory investigations should include moderately elevated 17-hydroxyprogesterone (17-OHP; concentration >6 nmol/L but <100 nmol/L). If basal levels of 17-OHP are normal but still clinically suspected, a corticotropin stimulation test will demonstrate elevated 17-OHP in affected patients. Exogenous sources of virilization should also be considered, especially in patients that demonstrate normal 17-OHP, luteinizing hormone, and dehydroepiandrosterone sulfate, and elevated testosterone. Dermal conversion of testosterone is more active in young children and should be considered if a child is in close contact with an exogenous androgen.
Adolescent male acne patients are more likely to present with acne fulminans generally between the ages of 13 and 22. Acne fulminans presents with acute onset of nodulocystic inflammatory lesions, fever, myalgia, arthralgia, and bone pain. Laboratory investigations demonstrate systemic involvement with leukocytosis, elevation of erythrocyte sedimentation rate, and occasionally, anemia, proteinuria, and microscopic hematuria. Bone involvement is commonly located at the sternum and clavicle but may occur at other sites. Generally, 50% of patients have lytic bone lesions. Less commonly, these patients may also present with erythema nodosum. There have been cases of acne fulminans with underlying Crohn disease, but this is rarely reported. There have also been alarming accounts of anabolic androgenic steroid–induced acne fulminans. Response to traditional antibiotic therapy is inadequate to control patients with acne fulminans. Initiation of oral steroid and low-dose isotretinoin over 3 to 5 months to avoid relapse is recommended. Refractory cases may respond to azathioprine or infliximab. In contrast, a similar acute onset without systemic involvement, called pseudoacne fulminans or acne fulminans sine fulminans, may be seen in male adolescents initiated on isotretinoin therapy. The entity may also be controlled with low-dose systemic corticosteroids 0.5 to 1.0 mg/kg for 4 to 6 weeks with slow taper and decrease of isotretinoin dosage to 0.5 mg/kg/d and slowly increased as steroids are tapered.
It is our differences that make us stronger, and our differences will expand our knowledge of the pathogenesis of acne. Although the understanding of the mechanism for the development of acne is in its relative infancy, as the understanding of the pathogenesis of acne expands, the differences in skin physiology between the sexes may alter the manner in which male patients are approached with acne medications. These differences may also lead to the development of new innovative treatment modalities that can target these differences.
Related posts:
 The Relationship of Proper Skin Cleansing to Pathophysiology, Clinical Benefits, and the Concomitant Use of Prescription Topical Therapies in Patients with Acne Vulgaris
Top Ten List of Clinical Pearls in the Treatment of Acne Vulgaris
Use of Oral Contraceptives for Management of Acne Vulgaris
Evaluation of Acne Scars
Physical Modalities (Devices) in the Management of Acne
The Relationship of Proper Skin Cleansing to Pathophysiology, Clinical Benefits, and the Concomitant Use of Prescription Topical Therapies in Patients with Acne Vulgaris
Top Ten List of Clinical Pearls in the Treatment of Acne Vulgaris
Use of Oral Contraceptives for Management of Acne Vulgaris
Evaluation of Acne Scars
Physical Modalities (Devices) in the Management of Acne
 When Acne is Not Acne
When Acne is Not Acne
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


