47. Ethnic Rhinoplasty
Paul N. Afrooz, Dean M. Toriumi
■ Rhinoplasty is becoming increasingly more common in nonwhite patients worldwide.
■ Most patients desire an improvement in their appearance, with preservation of certain ethnic features.
• This is accomplished through a highly individualized approach involving recognition of anatomic variations, familiarity with cultural aesthetics, an understanding of patients’ preferences.
■ Surgical objectives include:
• Nasofacial harmony
• Symmetry of the brow-tip aesthetic line
• Appropriate dorsal line shape
• Appropriate tip projection, rotation, and definition
• Appropriate base width and alar flare
• Functional breathing
PREOPERATIVE EVALUATION
■ Patient consultation with discussion of aesthetic preferences and cultural concerns. Assess patient expectations and preferences, and determine whether the goal is for Westernization of features versus maintenance of natural characteristics.
■ Complete problem specific and surgical history; history may greatly alter surgical plan
• Trauma or prior nasal or sinus surgery
• Previous alloplastic implant
• Injectable fillers in the nose
• Functional complaints
■ Physical examination
• Palpation of cartilaginous and bony structure, dynamic inspiration, endoscopy
■ Standardized photography (frontal, lateral, three-quarter, basal views)1 (see Chapter 3)
■ Three-dimensional stereophotogrammetry facilitates objective comparison of preoperative and postoperative results.
■ Digital image-morphing software2,3 allows direct communication of proposed changes to all parameters (dorsal height, nasal length, tip rotation/projection, and base width). Patients may comment on desired modifications based on the morphed image.
TIP: The use of a computer-imaging program can demonstrate potential changes preoperatively and aid in communication between patients and surgeons regarding expectations and possible outcomes.4
■ Facial analysis to assess for variation from the nonwhite aesthetic “norm.” Similar differences exist among people of same ethnic group.
• Recognition of each facial feature and how it relates to the nose is critical to achieve nasofacial harmony.
► Forehead slope/glabellar prominence
► Nasofrontal angle
► Intercanthal distance
► Upper lip length and contour
► Premaxillary position
► Dentition
► Chin position
INFORMED CONSENT
■ List exact procedure, including all planned types of grafts.
■ Location and laterality of harvest site
■ Possibility of banking unused cartilage behind the ear
■ Alternatives to surgery
■ Potential complications, including donor site morbidity and need for further surgery
PREPARATION
ANATOMIC VARIATIONS5–9
■ Skin is usually thicker, more sebaceous, and relatively inelastic in ethnic patients.
■ Fibrofatty layer is also thicker (2-4 mm) and more prominent over the lower lateral cartilages and between the medial crura. It plays a significant role in lack of tip definition. The soft tissue facet is often obtuse and filled with fat.
SENIOR AUTHOR TIP: Thick skin often requires making the nose larger (more projection) to stretch the envelope and allow underlying structure to provide definition.
Thinning of the skin and soft tissue envelope is often necessary in ethnic patients. Fat is evenly removed from the undersurface while taking care to preserve the subdermal plexus.
■ Alar base usually has an increased base width with insertion lateral to the medial canthal lines. There is excess flaring where the alae extend more than 2 mm lateral to the alar-facial groove.
■ A wide spectrum of dorsal morphology exists (low height in black and Asian nose, hump in Middle Eastern nose). Nasal bone length can also vary widely (Table 47-1).
Table 47-1 Specific Ethnic Characteristics
| Ethnicity | Characteristics |
| Black nose | Short nasal bones Wide nose Low dorsum Wide bimalar distance Horizontally oriented nostrils, wide base Deficient premaxilla Limited septal cartilage |
| Asian nose | Thick sebaceous skin Low dorsum Weak lower lateral cartilage Less septal cartilage Deficient premaxilla Wide nasal base Retracted columella |
| Middle Eastern nose | Long nasal bones Low radix Large hump Hanging columella Septal deviation |
Hispanic nose (types described by Daniel10) | Type I (Castilian): Normal radix height, high bridge, normal tip projection Type II (Mexican American)—most common: Low radix height, near-normal bridge, dependent tip Type III (Mestizo): Broad base, thick skin, wide tip Type IV (Creole)—predominantly black features: Broad, flat lower third, short columella, transversely oriented nostrils, flaring alae |
TIP: Weak cartilaginous structure can lead to a more pronounced effect on tissue healing. This highlights the importance in creating strong support for long-term results.
GRAFTING MATERIAL (see Chapter 27)
■ Nasal septum, auricular cartilage
■ Costal cartilage11 is stronger; therefore it can be cut thinner with less bulk in the nose. It has a lower vascular demand making it less likely to resorb. Surgeons are able to harvest a larger volume of material. Pain at donor site is decreased (compared to the ear) because less cautery is used.
TIP: Disadvantages to costal cartilage harvest (increased operative time, warping, and donor site morbidity) are minimized with experience.
■ Bone grafts include iliac bone and split calvarial grafts.
■ Irradiated rib may also be an option.
■ Types of allografts include: Silicone, ePTFE, and porous polyethylene.
• Advantages:
► Ease of use
► No additional surgical site
► Minimal change in operative time
• Disadvantages:
► Increased lifetime risk of infection
► Displacement/extrusion
► Thinning of skin over implant site
► Implant translucency and pain
TIP: Structural grafting can lead to nasal stiffness, which should be discussed with the patient during the initial consultation.
TECHNIQUE
PREOPERATIVE PLANNING
■ General anesthesia with oral endotracheal intubation for airway protection from blood and secretions; also allows costal cartilage harvest if indicated
■ Local anesthetic (1% lidocaine with 1:100,000 epinephrine) is injected before prepping and draping. This allows ample time for vasoconstriction. Injection also creates hydrostatic dissection for ease of elevation of mucoperichondrial flaps. Surgeons assess amount of available bony and septal cartilage by needle palpation at this time.
■ Infection prophylaxis with first-generation cephalosporin and fluoroquinolone if costal or auricular cartilage to be harvested. The entire face and intranasal area are prepared with dilute povidone-iodine, and the patient is draped to maintain sterility throughout the procedure. If cartilage is to be harvested, surgeons must change gloves to prevent contamination.
OPENING THE NOSE
■ Columellar (inverted-V, stairstep) incision made with a No. 11 blade. If deprojection is planned, incision is placed closerto tip lobule (below top of nostrils) (Fig. 47-1). For patients requiring increased projection, incision should be slightly below mid-columellar level and not close to the upper up.
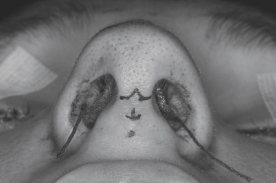
Fig. 47-1 Varying inverted-V columellar incision. Placed closer than normal to the tip lobule as the surgeon plans to deproject the nose.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


