Epidemiology of Breast Cancer: Incidence and Risk Factor
Jill R. Dietz
Chantal Reyna
Incidence, Mortality, and Survival
Breast cancer is the second most common cause of cancer globally and the most common cause of cancer in women, accounting for 12.3% of total cancers (1). When specifically looking at women, breast cancer has the highest incidence, accounting for 25.4% of new cancer diagnosis in the female population (2). In 2018, there were over 2 million new breast cancers diagnosed globally (1). Incidence ranges from 27 per 100,000 in Africa and Asia to 92 per 100,000 in the United States, a threefold difference between the lowest and highest countries. Although breast cancer is the 5th most common cancer death worldwide, it remains the most common cause of cancer mortality in less developed countries at 14.3% (3).
In the United States specifically, the average lifetime risk of breast cancer is 12.4%. Excluding skin cancer, breast cancer remains the most common cancer in females and responsible for the second highest cancer deaths. It accounts for 15.3% of new cancer cases. In 2018, there were 266,120 newly diagnosed invasive breast cancers with an additional 63,960 newly diagnosed carcinoma in situ (4,5). It is estimated that the new cases of breast cancer will rise to 271,270 in 2019. Although the mortality rates have decreased 39% from 1989 to 2015, a woman still has a 2.6% chance of dying from breast cancer. There were still 40,920 deaths from breast cancer in 2018 and 6.7% of all cancer deaths (4,6). Rates have been declining in older women and have remained steady in women younger than 50 years old (6).
There are over 3 million survivors in the Unites States, including those undergoing treatment and post treatment. According to the American Cancer Society, the relative 5-year survival from 2008 to 2014 for female breast cancer was 90% for all stages. A recent study confirmed that the 5-year survival was 90.2% in the United States, 89.5% in Australia, but only 66.1% in India when looking at cases from 2010 to 2014 worldwide (7). In the United States, survival rate for stage 0 or 1 breast cancer is near 100% compared to stage 3 which is 72% or stage 4 which is 22%. When evaluating for whether local, regional, or distant disease was present at diagnosis the rates look slightly improved (99%, 85%, and 27%, respectively) (6).
Changing Trends and Migration
While breast cancer incidence is stable or slightly increasing, the mortality rates are decreasing in high-income countries, mainly in Northern/Western European countries. In certain areas including France, Italy, Israel, Norway, and Spain, both incidence and mortality of breast cancer is decreasing. However, in other countries (Colombia, Ecuador, and Japan) incidence and mortality rates are climbing. There are some areas where mortality rates are rising such as in Brazil, Egypt, Guatemala, Mexico, and Moldova (8).
Incidence, mortality, and survival rates vary across the world and the trends are also changing. These changes can also be seen within individual migration. Individuals who move from a low-risk to a high-risk country change the risk of breast cancer within one or two generations. Specifically, Asian women who moved to the United States had increase breast cancer incidence after one or two generations (9). This suggests there may be some environmental factors contributing to the increased risk.
Risk Factors
Gender, Age, and Race
Breast cancer is 100 times more likely to be found in women than men. As a result, most research is based on women. However, male breast cancer makes up 1% of cases in the United States (10). In the United States, the incidence of male breast cancer has increased 0.8% per year, with 1.3 new cases per 100,000 from 2008 to 2012. Although both female and male breast cancer have increased incidence with age, male breast cancer does not show any difference of incidence based on race, and it presents at a more advance stage, with a
decreasing mortality rate (11). The rest of the chapter will focus primarily on female breast cancer in the United States.
decreasing mortality rate (11). The rest of the chapter will focus primarily on female breast cancer in the United States.
It has been shown that breast cancer incidence increases with age in both men and women. The median age of diagnosis for female breast cancer is 62 years old. When looking at age ranges, 46.3% of cases are diagnosed between the ages of 45 to 64 years old, with the highest number of cases found from 55 to 64 years old (5). The lowest number of cases are found from 20 to 43 years old. The median age of death is 68 years old, with the majority of deaths occurring at 65+ years old (5).
Incidence and mortality rates as well as other characteristics vary with race. Non-Hispanic white women have higher rates of breast cancer with Korean Americans having the lowest rates (Fig. 1-1) (4). African Americans have the highest incidence of breast cancer in the 40 to 50 year age group. The incidence rate in African American women has increase 0.3% annually whereas in has remained fairly stable in non-Hispanic white women (6). African Americans also have the highest 5-year mortality at 28.9 deaths per 100,000 persons and Asian Pacific Islanders have the lowest at 11.4 deaths per 100,000 persons (4,6,10). This can be partly explained as African Americans present with more advanced stages and disparities to health care access. However, when correcting for disparities, African Americans still have the highest mortality suggesting there are additional contributing factors (12,13).
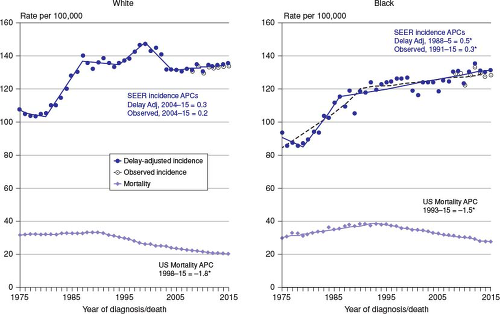 FIGURE 1-1 Breast cancer incidence and death rates in the United States by race. (Data from Noone AM, Howlader N, Krapcho M, et al., eds. SEER Cancer Statistics Review, 1975–2015. Bethesda, MD: National Cancer Institute. https://seer.cancer.gov/csr/1975_2015/, based on November 2017 SEER data submission, posted to the SEER web site, April 2018.) |
Early Life Events
During developmental periods (fetal, childhood, and adolescence), breast tissue may be more vulnerable to carcinogenesis (14,15).
Exposure in utero to diethylstilbestrol (DES), the first synthetic female hormone has been shown to have an increased risk for breast cancer, particularly after the age of 40 (16). While a European study did not show a difference between those exposed to DES in utero and those who were unexposed, a more recent 2011 study confirmed previous results that showed there was a risk of breast cancer after 40 years of age (17). Daughters of women who took DES while pregnant should be informed of their risks in the future.
Other in utero events have been associated with elevated risks of breast cancer. Twin pregnancy has shown a 1.2 times increase risk compared to a single live birth (18). Meanwhile, preeclampsia and eclampsia have also been associated with a lower risk of breast cancer (19,20,21,22).
Some studies have demonstrated that increased birth weight has increased the relative risk of breast cancer. Two meta-analyses showed that increased birth weight has an increased risk of breast cancer with one study showing up to 23% (19,23). In the United States, a more recent study meta-analysis of 34 studies Park et al. confirmed that that birth weight did increase risk of breast cancer, about 18% for those in the heaviest category (18). A Swedish study showed that increased birth weight for gestational age had an increased risk of breast cancer for those under 50 years old (24). Premenopausal risk for breast cancer has been shown to have increased with higher birth weights with a 5% increased risk per 500 g, but this was now shown to increase postmenopausal breast cancer risk (25,26,27). It is theorized that circulating maternal estrogens and IGF-1 may be responsible for the elevated risk. This has been documented in animal models (28,29).
Radiation exposure is a known risk factor for primary breast cancer. Ionizing radiation even at low doses increases the development of breast cancer (30,31). There is a higher risk of breast cancer when the age of exposure is less than 20 years old and less for older than 40 years old, and the risk lasts a lifetime (32,33). Based on the fact that both low-dose cumulative effect seen in atomic bomb and diagnostic radiation and high-dose effect with high cumulative doses seen in Hodgkin lymphoma have been shown to increase the risk of breast cancer, this has led to a theory where there is linear increase for low-dose cumulative dose up to 10 Gy where it flattens out, and then no or minimal increase at 40 Gy (34). Although ionizing radiation does increase the risk of primary breast cancers, adjuvant radiation therapy for de novo breast cancers treated after 45 years old of age is not associated with an elevated risk for a second primary breast cancer (34). Overall, younger age of radiation exposure, higher radiation dose, and longer follow-up demonstrate increases breast cancer risk.
Age of Menarche
It has been known that the age of menarche is linked to the risk of breast cancer. However, early menarche is associated with several other risk factors such as parity, age at first birth, adult height, and BMI which may confound the absolute risk (35). It has been shown that menarche at a young age increases breast cancer risk with a relative risk of 1.05 per year younger than the age of 13 (36). Ma et al. found that late menarche decreased the risk of both hormone receptor positive and negative breast cancers, but was more protective against hormone receptor positive cancer (37). Menstrual age was more associated with lobular rather than ductal carcinoma (35,38). Unfortunately, the age of menarche is decreasing. However, the prostate, lung, colorectal, and ovarian (PLCO) cancer screening trial has shown that menstrual age is becoming a less important risk factor and may have other influences as previously mentioned (35,39).
Age of Menopause
The age of menopause has been shown to influence the risk of breast cancer. There was no difference in risk where it was a surgically induced or natural menopause (35). The risk of breast cancer doubles each decade until menopause and then stabilizes, although it is still more common in postmenopausal women (40). PLCO trial demonstrated a relative risk of 1.29 for breast cancer in women who had menopause older than 55 years old compared to those less than 45 years old, with less than 45 years appearing to be protective (39). The risk increases 1.029 times for each year older than mean age of natural menopause (49.3 years); it doubles for every decrease after menopause. This is particularly true for estrogen-positive breast cancer and lobular carcinoma (39).
Reproductive History and Parity
Reproductive history and parity are standard portions of risk assessment for breast cancer. Early parity appears to be protective as individuals who had their first child prior to the age of 25 had a lower risk for breast cancer than those where were older than 30 years old and nulliparous (36). This association is seen only in hormone-positive breast cancer and ranges from 11% to 36% reduced risk (37,41). Later parity however increased risk of breast cancer up to 27% as well as increased the risk of hormone receptor negative breast cancer. Younger parity with additional births was protective against hormone-positive breast cancer regardless of breastfeeding, but later parity with additional births and no breastfeeding showed an increase risk of breast cancer (41). Although most studies show a decreased risk of breast cancer with parity in the long term, there is an interval increase in the peripartum risk and some data suggesting increased risk based on timing of multiple parity. There is a short-term increased risk associated with pregnancy, but postpartum there is a 5- to 10-year period of protection (42,43,44). One study even found that having more than one birth decreased the risk of cancer (45). However race and intervals between births may place a factor. Increased parity was shown to have increased risk for breast cancer in African American women younger than 45 years old, but a reduced risk for those older than 45 years old (46). In relation to intervals between births, a Finnish study evaluated the timing between pregnancy and number of pregnancies to find that having more than five children within 1-year intervals increased the risk of breast cancer compared to 3-year intervals. In terms of parity and abortion, a meta-analysis showed there was no risk of breast cancer as a result of abortion whether it was spontaneous or induced (47). This was further supported by the Committee of Gynecologic Practice, which stated no increased risk of breast cancer associated with abortion (48).
Breastfeeding
Breastfeeding has been shown to decrease the risk of breast cancer (25). Breastfeeding for at least a year has been shown to decrease risk of breast cancer, both for hormone-positive and hormone-negative subtypes (49). Some studies have shown that there is a 2% decrease in risk per 5 months of breastfeeding (25,50). Additionally, some studies suggest that a total year of breastfeeding either with a single birth or over several children, decreases the risk of breast cancer 4.3% (50,51). In a recent meta-analysis, breastfeeding was shown to be protective in estrogen receptor (ER)-negative and triple-negative breast cancer (50). The protection of breastfeeding from cancer is theorized to be influenced by alternating hormonal patterns, decreasing menstrual cycles, and inducing amenorrhea. This can decrease exposures to sex hormones which have been shown to increase breast cancer risk (52). Furthermore, it is believed that lactation exfoliates the breast and ductal tissue which can purge defective cells and induce apoptosis in potentially premalignant cells with damaged DNA at the end of lactation (25).
Nutritional Factors
Nonstarchy Vegetables
Although previous studies have eluded to a preventive factor with non-starch vegetables with high consumption, other studies have shown no association between starch consumption with breast cancer overall (25,53,54,55). When looking at dose-related intake, a meta-analysis has confirmed no significant association with 200 g intake per day and breast cancer risk in both pre- and postmenopausal women (25). Although the Nurse’s Health Study did not show any association between nonstarchy vegetables and ER-negative breast cancer, several other studies have (55,56). When stratified for hormone receptor status, several studies showed a decrease risk for ER-negative PR-negative breast cancer (55,57,58). When looking at total amount of vegetables, a pooling project of cohort studies showed that an intake of more than 300 g a day decreased the risk of breast cancer by 12% (55). It is thought that the phytochemicals in vegetables reduce epidermal growth factor (EGF), thus reducing ER-negative breast cancer which has higher amounts of EGF (55).
Dairy
A pooled analysis of several cohort studies did not show any association between dairy fluids or solids for 100 g per day intake and breast cancer, but more recent studies have found a protective factor of dairy products in premenopausal women (59). It has been shown that there is 5% decrease in risk of premenopausal breast cancer per 200 g intake of dairy products per day (25). Dong et al. performed a meta-analysis of 18 publications which also has demonstrated a decreased risk of premenopausal breast cancer when comparing higher to lower intake of total dairy products (60). Zang et al. performed a more recent and larger meta-analysis of 22 prospective cohorts in Western and Asian women and has found high dairy intake (>600 g/day) significantly reduced the risk of premenopausal breast cancer. It also has shown that yogurt and low-fat dairy products were the more significant dietary foods (61). However, there is no association seen between dairy products and the risk of postmenopausal breast cancer.
Carotenoids
It has been suggested that carotenoids decrease the risk of breast cancer. Clear evidence has demonstrated that higher levels of certain carotenoids such as circulating beta carotene, total carotenoids, and lutein have a protective benefit against breast cancer. Alpha carotene, beta cryptoxanthin, and lycopene have some evidence which suggests a decreased risk of breast cancer (62). This relationship appears to be more closely associated with ER-negative breast cancer. Several studies have shown that dietary beta carotene, diet alpha carotene dietary lutein/zeaxanthin, and circulating alpha carotene decrease risk of ER-negative breast cancer (62,63,64,65,66). A recent study, the EPIC study, has shown circulating alpha and beta carotene decrease the risk of ER-negative breast cancer and circulating lutein was protective for ER-positive breast cancer (64). It is suggested that carotenoids affect breast cancer risk through cell differentiation and apoptosis. They have antioxidant properties which help protect cells from DNA damage (67).
Calcium
Calcium rich diets are protective against pre- and postmenopausal breast cancer. Several studies have confirmed that high-calcium diets when compared to lower calcium diets decrease the risk of premenopausal breast cancer (68,69,70,71,72). There is a 13% decreased risk per 300 mg of calcium per day in premenopausal women and 4% in postmenopausal women (25). Calcium is a second messenger in cellular pathways affecting cell proliferation and apoptosis (73,74). It has been shown in rodents that calcium decreases fat-induced mammary proliferation which may decrease cancer cell proliferation (74).
Alcohol
Although not previously demonstrated, multiple studies have now shown an association between increased alcohol consumption and breast cancer (75,76,77,78,79). There is suggestion that it is a risk factor for premenopausal breast cancer, but a clear risk for postmenopausal breast cancer (80). When investigating dose-related alcohol use and breast cancer, there appears to be a significant risk factor in the United States for premenopausal breast cancer and
a significant factor in Europe and North American in postmenopausal women. In fact, a 5% increase in the risk for premenopausal breast cancer has been found when consuming more than 10 g of alcohol per day with beer being a higher risk factor than wine or spirits. In the postmenopausal population, a 9% increase of risk has been shown per 10 g of alcohol per day with wine being more of a risk factor (25,80). Additional findings support that alcohol was associated with ER-positive cancer in postmenopausal breast cancer (76,80,81,82). A pooled analysis has demonstrated increase in risk for ER-positive and PR-positive breast cancers with greater than 15 g of alcohol per day (80). A study by Schonfeld et al. shows that seven alcoholic drinks per week compared to no alcohol intake increased risk of postmenopausal women with relative risk increase based on parity (Table 1-1) (83). Research theorizes heavy alcohol use can lead to malnutrition and susceptibility to carcinogenesis. Rodent studies show alcohol can affect carotenoid metabolism and create free oxygen radicals, an already established protective factor for breast cancer (84).
a significant factor in Europe and North American in postmenopausal women. In fact, a 5% increase in the risk for premenopausal breast cancer has been found when consuming more than 10 g of alcohol per day with beer being a higher risk factor than wine or spirits. In the postmenopausal population, a 9% increase of risk has been shown per 10 g of alcohol per day with wine being more of a risk factor (25,80). Additional findings support that alcohol was associated with ER-positive cancer in postmenopausal breast cancer (76,80,81,82). A pooled analysis has demonstrated increase in risk for ER-positive and PR-positive breast cancers with greater than 15 g of alcohol per day (80). A study by Schonfeld et al. shows that seven alcoholic drinks per week compared to no alcohol intake increased risk of postmenopausal women with relative risk increase based on parity (Table 1-1) (83). Research theorizes heavy alcohol use can lead to malnutrition and susceptibility to carcinogenesis. Rodent studies show alcohol can affect carotenoid metabolism and create free oxygen radicals, an already established protective factor for breast cancer (84).
Related posts:
 Axillary Nodal Recurrence
Axillary Nodal Recurrence
 The Surgical Management of Locally Advanced and Stage IV Breast Cancer
The Surgical Management of Locally Advanced and Stage IV Breast Cancer
 Alternative Methods for Axillary Sentinel Lymph Node Dissection
Alternative Methods for Axillary Sentinel Lymph Node Dissection
 Optimizing Mastectomy Flaps Based on Breast Anatomy
Optimizing Mastectomy Flaps Based on Breast Anatomy
 Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
 Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


