Fig. 2.1
The global AD prevalence is based on the international study of asthma and allergies in childhood (ISAAC) phase I [4]
There have been several studies concerning the prevalence of AD in Japanese populations (Table 2.1) [6]. The prevalence is widely different among studies (Table 2.1) and ranges from 3.85 to 24.3% in age 6–10 years and 3.85 to 17.3% in age 12–13 years. The wide variations of the reported prevalence of AD are due at least in part to the fact that epidemiological studies of AD are influenced by a variety of factors, including year of survey, region, and methods of investigation [7]. A nationwide prevalence survey performed in Japan from 2000 to 2002 showed 11.8% in age 6–7 years [8] (Table 2.1). Prevalence in Tokyo obtained by the ISAAC core written questionnaire was 10.9–19.6% in 6–14-year-old schoolchildren (Table 2.1) [9]. A web-based study performed in 2012 showed 13.0% average prevalence in 6–12-year-olds [10]. In contrast to children, there are not many surveys of AD prevalence in adult populations. There was one in Japan that was a survey of students and employees at two universities. Prevalence ranged from 9.4% for participants in their 20s to 2.5% for participants in their 60s [11] (Fig. 2.3).
Table 2.1
AD prevalence as determined by Japanese studies
6–10 years (%) | 12–13 years (%) | 14–15 years (%) | ||
|---|---|---|---|---|
1981–1983 | Aichi | 3.85 | 1.96 | |
1990 | Osaka, questionnaire | 19 | 9.2 | 9.0 |
1992 | West Japan (11 prefectures, questionnaire) | 17.3 | ||
1993 | Hirosaki | 9 | 9.2 | |
1993 | Hamamatsu | 24.3 | ||
1995 | Nagasaki | 8.0 | ||
1996 | Ibaragi | 7.6 | ||
1992–1997 | Hiroshima, Asa area | 13.7 | ||
2001 | Hiroshima | 10.9 | ||
2001 | Maebashi | 9.9 | ||
2002 | Isahaya | 10.1 | ||
2002 | West Japan (11 prefectures, questionnaire) | 13.8 | ||
2000–2002 | All Japan, eight cities | 11.8 | 10.6 | |
2005 | Tokyo | 19.6 (6 years old) | 13.6 (12 years old) | 10.9 (14 years old) |
2012 | Web-based study | 13.0 | ||
2.3 The Prevalence of AD Differs Within a Country
Variations in AD prevalence are observed not only between countries but also within countries. This is evident in the ISAAC phase III study [5] (Fig. 2.4) and in Japanese domestic studies (Table 2.1). A number of studies show that the geography and climate influence the development of allergic diseases. Weiland et al. [12] studied AD prevalence in 12 countries in Western Europe and found that it was positively associated with latitude and negatively associated with mean annual outdoor temperature. Different prevalence in regions with distinct climates was also observed within Japan. While average prevalence of childhood AD in mainland Japan is 12–13%, it drops by half on Ishigaki Island, which is remotely located in a subtropical area of Japan [13] (Fig. 2.5). The comparatively lower rate was also observed in another remote subtropical island, Ogasawara [14] (Fig. 2.5). In Ogasawara, AD prevalence in preschool, elementary school, and junior high school students combined was 4.3%; individual age-group prevalences were 7.1% for preschool, 2.8% for elementary school, and 2.3% for junior high school. The prevalence of AD was evidently lower in Ogasawara Island than in mainland Japan. Both islands are at a similar latitude to Taiwan, where prevalence is also lower than Japan (Fig. 2.1). The lower prevalence in these subtropical islands is consistent with observations in Western Europe [12]. Nevertheless, the possibility cannot be excluded that the lower prevalence in these subtropical islands may be attributed to not only climate conditions such as higher temperature and humidity but also different lifestyles of children there compared to children from other regions of Japan. On the islands, children spend shorter amounts of time inside watching TV and more time exercising outside instead [14].
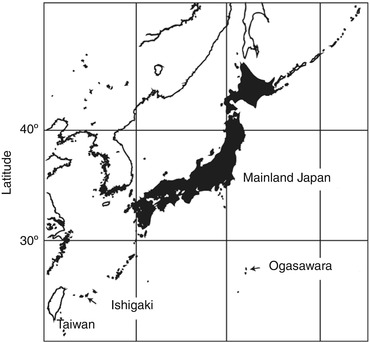
Fig. 2.4
Diversified AD prevalence within countries. Each black dot represents a center or a region that participated in the ISAAC study in each country. Countries with more than three centers are depicted. Data were adapted from [5]
Fig. 2.5
A map of Japan. Ogasawara and Ishigaki islands are located at a similar latitude to Taiwan
2.4 The Natural History of Atopic Dermatitis
In general, most children who suffer from AD start presenting skin symptoms within the first months of life. Around 60% of children will outgrow the disease or become free from symptoms before puberty [15–17]. A significant number of patients will sequentially develop other allergic diseases such as allergic rhinitis and asthma. In fact, AD increases the risk of developing asthma to ~50% and the risk of developing allergic rhinitis to as much as 75% [18–20]. This typical sequence of development of allergic diseases during childhood is called “atopic march” [21, 22]. Futamura et al. reported that among 27,389 children aged 6–14 years, 14.0%, 41.6%, and 31.3% of children had symptoms of asthma, allergic rhino-conjunctivitis, and atopic dermatitis, respectively. While 43.1% of the children in this study had more than one of the symptoms during the past 12 months, 2.2% had all three symptoms.
AD affects up to ~20% of children during infancy and early childhood [9, 23]. Understanding of occurrence and progression of infantile atopic dermatitis is based on a cohort study of infants aged 4 months to 3 years reported by the Health and Labour Science Research, from 2006 to 2008, in the cities of Yokohama, Chiba, and Fukuoka. The report shows that 16.2% of ordinary infants who received a medical examination at 4 months of age developed atopic dermatitis. Atopic dermatitis regressed in 50% of the 4-month-old patients before the age of 18 months, indicating an extremely dynamic progression of atopic dermatitis in infancy [24].
AD affects 2–10% of adults (Fig. 2.3) [9, 23], which is much lower than the rates in children (7–19%) (Table 2.1). A hospital-based investigation showed that the number of AD patients gradually decreases from childhood to adolescence and abruptly drops in the fourth decade of life. After that, the prevalence again gradually decreases with age (Fig. 2.6) [23, 25]. A caveat of this data is that investigation took place at clinics or hospitals. Diagnosis was based on direct examination, and therefore it was more reliable than questionnaire-based study, but the reported prevalence is open to influence by behavioral factors; also, the total number of patients who visited hospitals and clinics is inconsistent between age groups (Fig. 2.6).
Fig. 2.6
Age distribution of patients in dermatology clinics in Japan [25]. Among 67,448 patients, 6733 were diagnosed with AD
2.5 Genetic Factors Associated with Childhood Atopic Dermatitis
A number of studies have demonstrated that there is a strong genetic predisposition for AD. Studies in twins clearly imply the presence of genetic effects in the development of AD and allergic diseases [26]. For instance, the pairwise concordance rate of AD in monozygotic twins was significantly higher (72%) than in dizygotic twins (23%) [27]. In addition to twin studies, genetic linkage analysis and association studies have also revealed the genetic background of AD. A notable example is the profilaggrin/filaggrin gene (FLG) [28]. Loss-of-function mutations in FLG account for 40% of the total mutations in AD patients [29]. FLG mutations are found in 10–50% patients with AD [28, 30, 31] and found in 9% of the normal population [29, 31]. The mutation is much more frequent (~50%) in European patients with moderate to severe AD than in Chinese patients (27%) [29]. In Japan, FLG mutations were found in about 27% of AD patients, while the same mutations are found in 3.7% of the general population [32, 33]. In addition to varying frequencies, FLG mutations have a wide spectrum. Mutations found in European AD patients are not common in Japanese patients. Mutations in Japanese patients are different from those of Chinese patients [34]. FLG mutations are likely specific to each population. The different genetic background between different populations might partly account for differences in prevalence between countries. FLG is the most influential gene for developing AD within those identified so far. Nevertheless, the frequency of FLG mutations in mild to moderate AD patients (~15%) is not as high as that in moderate to severe patients (~50%) [35]. This seems to indicate that FLG deficiency alone does not sufficiently explain genetic predisposition toward the disease and that other important genetic or nongenetic factors are involved in disease onset.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


