This review discusses key diagnostic points and treatment guidelines for compression neuropathies of the wrist, forearm, and elbow. Recent treatment progress is reviewed, controversies are highlighted, and consensus is summarized. Limited or mini-open releases and endoscopic carpal tunnel releases are considered equally safe and efficient. Both methods are currently mainstays of surgical treatment.
Key points
- •
Carpal tunnel syndrome (CTS) is diagnosed by sensory disturbance and weakness in muscles of the median nerve innervation. Phalen and Tinel signs are indicative of nerve problems but are not positive in all patients. The wrist compression test is more sensitive than those 2 tests. Limited or mini-open (2–3 cm incision) releases and endoscopic carpal tunnel releases (ECTRs) are equally safe and effective. Both methods are mainstays of surgical treatment. The choice depends on surgeon preference. Classic open release method has largely been abandoned.
- •
The key to a thorough decompression of ulnar nerve in cubital tunnel is to make sure all possible sites of compression are released. In a majority of the cases, in situ decompression is sufficient and can be achieved through a small incision or mini-incision or endoscopically; subcutaneous anterior transposition does not further improve outcomes. Anterior transposition is indicated during revision surgery or if the ulnar nerve is severely compressed with scar formation in the cubital tunnel.
- •
Median nerve compression by pronator teres, posterior interosseous nerve (PIN) compression, radial nerve compression in the proximal forearm, or ulnar nerve compression at the Guyon canal are less often seen. Surgical release of nerve at the compression sites is indicated when conservative treatment fails.
- •
Wartenberg syndrome (compression of the superficial radial sensory nerve) and anterior interosseous nerve (AIN) syndrome tend to resolve spontaneously.
Introduction
Compression of a segment of a peripheral nerve disturbs electrophysiologic conduction distal to the site of compression and increases intraneural pressure; prolonged or severe compression can result in structural degeneration or destruction of the nerve. Clinically, these pathologic changes lead to pain, sensory disturbances, and loss of normal motor function. The most common sites of compression in the forearm and wrist are the median nerve under the transverse carpal ligament and the ulnar nerve at the elbow. Less common compression sites are AIN, ulnar nerve at the wrist, radial nerve at the radial tunnel in the proximal forearm, PIN, and superficial sensory branch of the radial nerve. Because of their functional importance and higher prevalence, most investigations have been focused on median nerve compression at the carpal tunnel and ulnar nerve compression in the cubital tunnel.
Introduction
Compression of a segment of a peripheral nerve disturbs electrophysiologic conduction distal to the site of compression and increases intraneural pressure; prolonged or severe compression can result in structural degeneration or destruction of the nerve. Clinically, these pathologic changes lead to pain, sensory disturbances, and loss of normal motor function. The most common sites of compression in the forearm and wrist are the median nerve under the transverse carpal ligament and the ulnar nerve at the elbow. Less common compression sites are AIN, ulnar nerve at the wrist, radial nerve at the radial tunnel in the proximal forearm, PIN, and superficial sensory branch of the radial nerve. Because of their functional importance and higher prevalence, most investigations have been focused on median nerve compression at the carpal tunnel and ulnar nerve compression in the cubital tunnel.
Median nerve compression at the wrist: carpal tunnel syndrome
CTS is the most common compression neuropathy. A review of authors’ surgical cases in the past years indicated that 116 (63.7%) had CTS of 182 patients with compression neuropathy in wrist, forearm, and elbow ( Table 1 ).
| Compression Neuropathies | Number (%) |
|---|---|
| CTS | 116 (63.7) |
| AIN syndrome | 0 (0) |
| Pronator syndrome | 2 (1.1) |
| Cubital tunnel syndrome | 52 (28.6) |
| UTS | 3 (1.6) |
| RTS | 4 (2.2) |
| PIN syndrome | 0 (0) |
| Wartenberg syndrome | 5 (2.8) |
Diagnosis: Carpal Tunnel
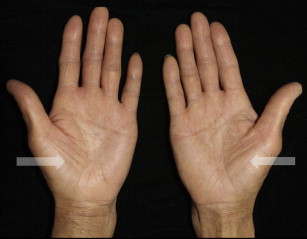
Patients predominantly complain of paresthesias or numbness, or both, in the area supplied by the median nerve, at the volar aspect of the thumb, index, long, and radial side of ring fingers. Patients frequently note nocturnal symptoms. The paresthesias may be aggravated on wrist movement or prolonged wrist posture in a bent position, such as when holding a baby or driving a car. As the disease progresses, patients may describe weakness of grasp and pinch and, later, atrophy of the thenar muscle ( Fig. 1 ). Thumb opposition becomes weak because of weakness of the opponens pollicis. Median nerve–innervated lumbricals may also become atrophic. Because all of these clinical manifestations are also seen with proximal median nerve compression, clinically, attention should be paid not to mistakenly diagnose nerve compression caused by cervical disk herniation, thoracic outlet structures, and median nerve compression in the forearm and at the elbow as CTS.
The Phalen test (wrist flexion test) or reverse Phalen test is frequently positive. The Tinel sign (ie, nerve percussion test) is also frequently positive. Other tests can be useful, including the wrist compression test, tourniquet test, closed fist test, flick sign, and hand elevation test. The most sensitive test is the Phalen test, whereas Tinel sign is the most specific yet the least sensitive. The positive rate of Tinel sign was 81.9%, but that of Phalen test was 53% in the authors’ patients. Popinchalk and Schaffer reviewed the literature and reported that the sensitivity and specificity of Phalen test are 46% to 80% and 51% to 91%, respectively, and of the Tinel sign 28% to 73% and 44% to 95%, respectively. The carpal compression test was more specific (90%) and more sensitive (87%) than the Phalen test and the Tinel sign. The diagnosis is primarily a clinical one based on a combination of symptoms and characteristic physical examination findings.
In 2006, Graham and colleagues performed a literature review that yielded 6 clinical criteria (nocturnal numbness, median nerve paresthesia, thenar muscle atrophy, positive Phalen test, positive Tinel test, and loss of 2-point discrimination [2PD]) that proved to correlate positively with a diagnosis of CTS. They stated that the value added by electrodiagnostic testing was minimal. Electrodiagnostic testing, however, is helpful in confirming the diagnosis, assessing the degree of nerve compression to predict the rate of recovery, differentiating from other clinical conditions, and eliminating coexisting lesions. Similar to all other diagnostic tests, false-positive and false-negative results occur. The false-negative rate of nerve conduction studies has been reported to be between 16% and 34%. No significant relationships exist between nerve conduction study results, symptoms, and function in patients with CTS.
MRI generates images of high soft tissue contrast in the carpal tunnel and is a sensitive diagnostic tool but it is rarely used, because clinical tests are sufficient for making the diagnosis. Ultrasound is easy to perform and used as a first-line tool to assist diagnosis. Injection of local anesthetic into the carpal tunnel can help eliminate the possibility of other syndromes, especially cervical disk or thoracic outlet syndrome.
Treatment: Carpal Tunnel
Nonoperative treatment options range from wrist splinting to corticosteroid injections. If the symptoms are mild and there is no thenar muscle atrophy, splinting the wrist in neutral or serial steroid injections frequently decreases symptoms, at least transiently. Corticosteroid injection is used by some surgeons. A few studies show that it improved the symptoms 1 month after injection, but 2 local injections do not have added benefit compared with 1 injection. A recent study showed that 30 of the 120 patients (25%) had a good outcome with a single injection, 11 patients (9%) needed a second injection, and 5 patients (4%) needed a third injection. Of patients with an initial good treatment response, 28 (52%) had a good outcome after 1 year compared with 18 (27%) who had an initially moderate or no response to treatment. One-third of patients had a long-term beneficial effect from corticosteroid injection, mostly when they had a good initial response. If signs and symptoms persist or progress after conservative treatment, especially if thenar atrophy develops, surgical decompression of the median nerve is indicated. For acute CTS after trauma, such as carpal bone dislocation, crush injury, or forearm compartment syndrome, immediate surgical release is always indicated.
Classically, the open technique is a standard practice. Under direct visualization through a large incision, the transverse carpal ligament is divided and the nerve decompressed. Over the past 20 years, surgical releases with smaller incisions (termed limited open or mini-open ) were popularized to minimize surgical morbidity and expedite return to work. Currently, limited open carpal tunnel release (OCTR) is a common practice ( Fig. 2 A ). Fewer surgeons now use tradition carpal tunnel release through a large incision.
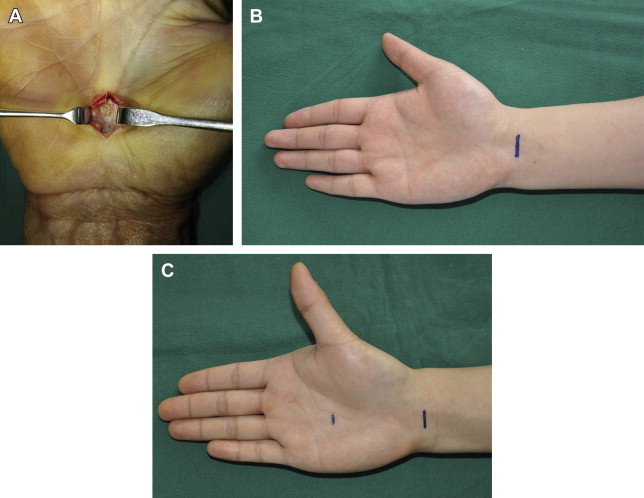
In 1989, Okutsu and colleagues described an ECTR technique using a single small incision 3 cm proximal to the wrist crease. They released the transverse carpal ligament longitudinally under endoscopic visualization using a hook knife. Chow introduced a technique using 2 skin incisions, with 1 incision just proximal to the wrist flexion crease ulnar to the palmaris longus tendon, and a second longitudinal incision 4 to 5 mm distal to the distal edge of the transverse carpal ligament. In 1993, Agee and colleagues modified this into what is called the Agee technique by using a single incision but introduced a trigger-deployed blade system to improve safety of the procedure.
Endoscopic techniques avoid midpalm incisions, preserving the palmar musculature and skin (see Fig. 2 B, C). Their shorter incisions also mean less scar tenderness and pillar pain. The disadvantages of ECTR are its learning curve and higher cost.
Multiple randomized controlled trials showed limited open procedure and the endoscopic approach to have similar rates of complications and parallel functional recovery. A 2004 meta-analysis of 13 randomized clinical trials by Thoma and colleagues compared OCTR with ECTR and analyzed data pooled from 3 studies without a significant difference observed between the 2 techniques. Immediate postoperative advantages of the endoscopic technique in grip strength and pain relief disappeared after 12 weeks. In a recent study, 52 patients with bilateral CTS had 1 hand randomized to undergo endoscopic release and the other to undergo mini-incision release. Despite similar improvements in subjective scores after endoscopic and open techniques at 3 months postoperatively, a majority of patients preferred the endoscopic technique because of the smaller scar and less pillar pain. Meta-analysis performed on 3 studies slightly favors ECTR in terms of symptom severity scores and functional scores at 12 weeks. Atroshi and colleagues compared the outcome of carpal tunnel release with 2 different techniques in 128 patients, showing carpal tunnel release with endoscopic and midpalm mini-incision having no difference in improvement in symptoms and hand-related disability over a 5-year follow-up. Recent reports about outcomes of these methods are detailed in Table 2 .
| Authors and Years | Number of Cases | Methods | Subjective Recovery | Complications | Authors’ Comments or Suggestions |
|---|---|---|---|---|---|
| Nakamichi et al, 2010 | 39 | Limited OCTR | The satisfaction was 4.7 at 104 wk (0–5 on VAS). | No | Limited OCTR had no complications, but earlier functional return seen in percutaneous CTR. |
| Vasiliadis et al, 2010 | 37 | ECTR | The DASH score was 20.7 ± 1.6 at 1 y. | Transient neurapraxia in 3 (8.1%) and slight scar hypersensitivity with paresthesias in 2 (5.4%) cases. | ECTR provides a faster recovery for the first 2 wk, with faster relief of pain and faster improvement in functional abilities. |
| Eisenhardt et al, 2010 | 170 | ECTR | Overall satisfaction is more than 4.5 at 6–89 mo by the BCTQ. | No | The endoscopic 1-port method is a low risk procedure with a low morbidity. |
| Beck et al, 2011 | 358 | ECTR | All patients reported major or complete relief of symptoms, including pain and numbness. | Transient neurapraxia in the long and ring web space in 1 (0.28%) case. | A learning curve for ECTR was present. Patients may be at a higher risk of conversion to OCTR during the learning period; nevertheless, there was no increased morbidity with ECTR. |
| Ritting et al, 2012 | 94 | Limited OCTR | The Levine-Katz score was 16.6 ± 5.5 at 6–12 wk. | Wound dehiscence was observed in 1 (1.1%) case. | Removal of a bulky dressing after limited OCTR and using an adhesive strip at 48–72 h causes no wound complications and results in equal short-term outcome. |
| Becker et al, 2012 | 66 | Limited OCTR | The DASH score was 9.9 ± 9.0; the satisfaction was 9.1 (with a 10-point scale) at 6 mo. | Not reported. | Actual relief of symptoms with limited OCTR matched patients’ expectations in an employed population. Satisfaction with treatment correlated with relief of symptoms. |
| Aslani et al, 2012 | 32 | ECTR | The satisfaction level of 2 techniques reached more than 90% at 4 mo. a | Pillar pain in 1 (3.1%) case. | The 2 techniques have better early satisfaction rates compared with regular open incision but no difference between the 2 techniques after 4 mo. |
| 28 | Limited OCTR | No | |||
| Zyluk & Puchalski, 2013 | 386 | Limited OCTR | The Levine-Katz symptom score was 1.4. Function score was 1.6–1.8 at 6 mo. | Superficial wound infection in 7 (1.8%) patients. Mild regional pain in 2 (0.5%) patients. | Age of patients has no significant effect on the effectiveness of surgical treatment of CTS. Patients older than 65 y, however, showed less improvement of the power of the hand |
| Louie et al, 2013 | 113 | Limited OCTR | The Levine-Katz score was 1.3–1.6. 13% Of patients had a poor symptom score; 26% had a poor function score at 13 (11–17) y. | Not reported. | At an average of 13 y after OCTR, a majority of patients are satisfied and free of symptoms of CTS. |
| Kang et al, 2013 | 52 | ECTR | BCTQ-S: 1.5 BCTQ-F: 1.5 DASH score: 11.3 at 3 mo. | No | The 2 techniques had comparable early subjective outcomes. A preference is determined by scar or pillar pain after an open technique and transient worsening of symptoms from the endoscopic technique. |
| 52 | Limited OCTR | BCTQ-S: 1.4 BCTQ-F: 1.7 DASH score: 10.8 at 3 mo | No |
a Based on the quintet symptoms, scar pain, scar appearance, and quantitative satisfaction.
In the authors’ practice, the mini-OCTR is preferred. A 2- to 3-cm incision is made directly above the transverse carpal ligament. Such an incision usually is sufficient to expose and release the ligament. Care is taken to preserve any median nerve branches over or through the transverse carpal ligament. The incision is closed with absorbable suture and immediate postoperative motion is encouraged. The authors agree that both mini-open and endoscopic approaches provide an excellent outcome. Therefore, the decision as to which technique should be performed should be left up to patient and surgeon, depending on training and experience. The authors’ colleagues are split into those who perform ECTR and those who perform limited OCTR. No one continues with the conventional large open incisions for carpal tunnel release. In the authors’ experience, the surgical times for ECTR and limited OCTR are similar and ECTR is safe if a surgeon confirms the structure of transverse carpal ligament before cutting. In those cases of severe symptom, severe muscle atrophy, and suspicion of other causes of compression, OCTR is preferred by all surgeons in the authors’ group.
Recently, ultrasound is used in the treatment of CTS. McShane and colleagues and Rojo-Manaute and colleagues reported the new technique of sonographically guided percutaneous needle release of the carpal tunnel and ultraminimally invasive carpal tunnel release, respectively. New devices have also been developed in recent years. McCormack and colleagues developed the MANOS device (Thayer Intellectual Property, Inc., San Francisco, CA) to divide the transverse carpal ligament using wrist and palm skin punctures. Preliminary results suggest this device as safe and effective. Pereira and colleagues introduced a modified Tsai 2-portal technique, creating a “fixed surgical tunnel” for decompression and a custom-made plastic tube used to check the quality of the release. Fechner and colleagues developed a new guiding cannula with raised borders to prevent accidental injury to the median nerve. Ip and colleagues used a new single-portal technique with instruments originally designed for endoscopic cubital tunnel release and reported no neurovascular or tendon injuries.
Complications in Carpal Tunnel
The complications of carpal tunnel release include infection, hypertrophic scar, scar tenderness, neuropraxias, and injury to nerve, artery, and tendon. Benson and colleagues reviewed 80 publications from 1966 through 2001. They found complication rates for carpal tunnel release, through either an endoscopic or open approach, to be very low. The incidence of structural damage to nerves, arteries, or tendons is 0.49% during OCTR and 0.19% during ECTR. Major nerve injuries were seen in 0.13% for ECTR and 0.10% for OCTR patients. ECTR had a rate of 0.03% for digital nerve injuries and 0.39% for OCTR. Arterial arch injuries occurred in 0.02% of the ECTR patients, with no cases in the OCTR patients. The most striking difference after open or endoscopic approach was in the rate of transient neuropraxias, which were reported in 1.45% of ECTR cases compared with 0.25% of OCTR cases. OCTR had more wound problems, such as infection, hypertrophic scar, and scar tenderness. The American Academy of Orthopaedic Surgeons report found 8 studies regarding wound-related complications, with 7 of 8 favoring ECTR, but the report failed to show a statistical difference in general complications or infection.
Pillar pain (the pain around the surgical incision of the carpal tunnel area) is relatively frequent after surgery ( Fig. 3 ). Its cause remains unknown although neurogenic inflammation is a possible cause. In the authors’ department, 30 cases after OCTR were followed for 10 to 30 months between December 2006 and October 2008; 11 cases of numbness and 8 cases of pillar pain around the incision were found. The analysis showed the length of incision positively correlated with the area of pillar pain; the type of approach (distal-mini or proximal-mini incisions) had no correlation with the presence of pillar pain. Cellocco and colleagues reported that mini-incision carpal tunnel release (<2 cm incision) showed advantages over standard technique (3–4 cm incision) in pillar pain. The treatment of pillar pain includes rest, bracing, and physiotherapy; however, all have uncertain effects and the pain can last quite long.

Prognosis and Recovery: Carpal Tunnel Release
Louie and colleagues followed 113 cases of OCTR for an average of 13 years and concluded that a majority of patients are satisfied and free of symptoms. In a prospective study of Tan and Tan of 74 cases, 72% showed complete symptomatic relief, 74% showed improvement in function, and 66% showed gain in grip strength; overall, 82% were very satisfied with the results at 6 months after surgery. Additionally, they found older patients and patients with weakness in muscle power had poorer outcomes. Higher preoperative symptom severity and functional severity scores were also associated with less improvement in symptoms and function, respectively. Zyluk and Puchalski reported patients older than 60 years showed less improvement in total grip strength of the hand. Cowan and colleagues found that job type is the most important determinant of return to full work after surgery, but that psychological factors, such as patient expectations, catastrophic thinking, and anxiety in response to pain, also play a role. Follmar and colleagues reported that patients receiving narcotic pain medication chronically for nonhand pain experienced a longer recovery period but ultimately achieved the same outcomes as patients without chronic pain.
The authors examined recovery of pinch strength in 31 patients having OCTR between 2008 and 2011. The pinch strength of all the cases did not return to normal 1 to 3 years after surgery; the recovery level of the pinch strength correlated significantly with the severity of muscle atrophy and severity and duration of compression before surgery. Subjective scores, however, such as Disabilities of the Arm, Shoulder, and Hand (DASH) scores, do not show patient dissatisfaction. All patients satisfied with the surgery and had remarkable improvement in function. After carpal tunnel release, subtle impairment of nerve and intrinsic muscle function can persist for years postoperatively.
Revision Surgery for Carpal Tunnel Release
Carpal tunnel release is one of the most frequently performed hand operations. Persistent, recurrent, or new symptoms after carpal tunnel release may require revision surgery. Revision surgery is indicated if there is only temporary or partial improvement in the symptoms or when classic carpal tunnel symptoms persist postoperatively. The surgical approach is to extend the previous incision into normal tissue to allow proximal or distal identification of the median nerve. The transverse carpal ligament is explored, and if the transverse fibers are remaining or reconstituted flexor retinaculum, these structures should be divided. Scar formation is frequent and can be severe and compressive to the nerve. A neurolysis may be indicated in these cases. Several procedures may help protect the nerve from recurrent scar, including vascularized soft tissue coverage (hypothenar fat pad flaps and synovial flaps) or autologous (vein grafts) or synthetic nerve wraps. Strickland and colleagues reported excellent results in 58 patients with 62 wrists who underwent revision carpal tunnel surgery using the hypothenar fat pad flap, with 37 of the 43 patients returning to their presurgery employment. Tollestrup and colleagues reported hypothenar fat pad flap can provide protective covering and a gliding surface for the median nerve. Chrysopoulo and colleagues modified this technique, so that the hypothenar fat pad transposition flap provides a reliable source of vascularized local tissue. Synovial flaps are frequently used. Vein wrapping and synthetic nerve conduit wrapping are additional methods for preventing scarring of the nerve.
Median nerve compression at the forearm and elbow
Pronator Syndrome
From the elbow down to the forearm, the median nerve is located anterolateral to the brachial artery, passes deep to the ligament of Struthers (if present), and continues into the antecubital region. The ligament of Struthers (present in approximately 1% of the population) is an anatomic variant that extends from a small, vestigial supracondylar process on the anteromedial diaphysis of the humerus to the medial epicondyle.
Pronator syndrome is the compression of the median nerve as it passes between the 2 heads of the pronator teres muscle. Pronator syndrome is characterized by vague volar forearm pain, with median nerve paresthesias and minimal motor findings. Despite its name, the nerve can also be compressed beneath the proximal arch of the flexor digitorum superficialis (FDS), bicipital aponeurosis, the Struthers ligament, or an accessory head of the flexor pollicis longus (FPL) (ie, the Gantzer muscle).
Diagnosis: Pronator
Pronator syndrome typically presents as insidious pain in the volar forearm, grip weakness, and paresthesias in the median nerve distribution in the digits and thenar eminence. The symptoms are exacerbated with repetitive pronation and supination movements. Patients typically do not report nocturnal symptoms because wrist flexion is not a cause. The diagnosis can be challenging because symptoms are similar to those of CTS. Pronator syndrome may be suspected in patients with a history consistent with CTS without demonstrable provocative signs (Tinel and Phalen signs) over the carpal tunnel. Unlike CTS, patients with pronator syndrome may report decreased sensation in the proximal thenar eminence, the distribution of the palmar cutaneous branch of the median nerve, which originates distal to the site of compression. This is the major sign differentiating the 2 syndromes clinically.
The distinctive physical examination for pronator syndrome is tenderness over the pronator teres muscle approximately 6 cm distal to the elbow crease and 4 cm lateral to medial epicondyle. The tenderness in the forearm is aggravated by provocation tests, including resisted forearm pronation (pronator teres), resisted elbow flexion with the forearm supinated (bicipital aponeurosis), and resisted flexion of the middle finger proximal interphalangeal joint. If the forearm is placed in maximum supination with the wrist in a neutral position, pressure over the leading edge of the pronator teres muscle produces paresthesias in the median sensory area. The scratch collapse test is often positive.
In a majority of patients, electrodiagnostic testing is normal; however, it may be helpful to rule out other sites of compression in patients with distal sensory symptoms. Radiographs of the elbow can identify the rare supracondylar process that may indicate compression under the Struthers ligament. Ultrasound or MRI can be used to look for extrinsic causes, such as a tumor or hematoma.
Treatment: Pronator
Conservative treatment with immobilization, physical therapy, a course of anti-inflammatory medication, and local injections are used when the symptoms are mild or duration of the disease is short. Longstanding symptoms warrant surgical treatment. Pronator syndrome is a controversial diagnosis and is typically treated nonsurgically. Surgical indications for nerve decompression include persistent symptoms for greater than 6 months. In the authors’ practice, surgical decompression is rarely indicated because the symptoms disappear with conservative treatment for 4 to 10 weeks. Surgery may be considered in patients who remain persistently debilitated for more than 6 months despite thorough nonsurgical treatment.
Surgical decompression is classically approached through an incision starting at the antecubital fossa and extending distally to the middle of the forearm for approximately 10 cm—this exposure provides excellent visualization of all potential sites of compression. However, in most patients, the tenderness point is localized 5 to 7 cm distal to the elbow. Therefore, an incision of 5 cm is sufficient for releasing the bicipital apooneurosis, two heads of the pronator tere and the arch of the FDS. The exploration is directed towards the ligament of Struthers using a smaller incision, if compression is suspected at this site according to the site of tenderness and presence of a supracondylar process on the anteromedial diaphysis of the humerus on radiographs. After surgery, patients begin exercise to regain full elbow extension with forearm supination after surgery. Patients are allowed full use of the hand and return to work without restrictions 6 to 8 weeks after surgery.
Hartz and colleagues reported that 28 (78%) of their 36 patients had excellent or good outcomes with an average of 18 months’ follow-up after surgical decompression. Zancolli and colleagues recently described a surgical technique that uses a mini-invasive approach to release the deep fascia of the superficial head of the pronator teres muscle and reported a 93% success rate in patients. Lee and colleagues reported an endoscopically assisted pronator release in 13 patients. All patients had improvement in their DASH scores after surgery; 8 of the 13 had complete resolution of symptoms, whereas 3 had residual arm discomfort.
Anterior Interosseous Nerve Syndrome
The AIN may be compressed by the tendinous origin of the deep head of the pronator teres, other variant tendinous structures, fibrous bands, or collateral vessels. Spontaneous and traumatic causes have been described.
Diagnosis: Anterior interosseous nerve
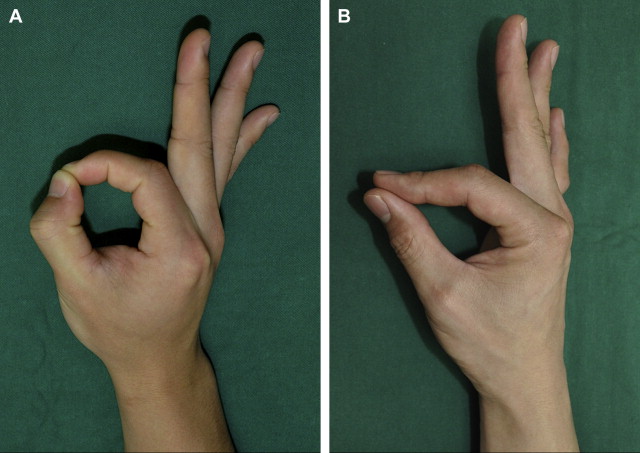
AIN syndrome is manifested as vague forearm pain and spontaneous loss of function of any or all of the AIN-innervated muscles. AIN innervates forearm flexor muscles except those innervated by the ulnar nerve. Therefore, weakness of power of the innervated muscles is common. Initial complaints include forearm pain and clumsiness with fine motor skills, such as writing and pinching. The FDP function of the middle finger may be preserved because of cross-innervation by the ulnar nerve. Because the AIN does not innervate the skin, the syndrome is not associated with any loss of sensibility. A characteristic finding in physical examination is a patient’s inability to make a rounded O between the thumb and index finger when asked by an examiner to flex the thumb interphalangeal joint and index finger distal interphalangeal joint ( Fig. 4 ).
AIN syndrome does not have a clear cause. It is most commonly attributed to a postinfectious neuritis or a compression of the AIN after it branches from the median nerve under the leading edge of the FDS origin. In most cases, it is the result of neuritis rather than being a mechanical compression. Electrodiagnostic studies serve an important role in the diagnosis because they can support the diagnosis and assess the severity of the neuropathy. Imaging studies, such as MRI, are not commonly used in the diagnosis of AIN syndrome.
Parsonage-Turner syndrome (brachial neuritis) should be considered in the differential diagnosis in patients with AIN syndrome. These patients typically have a history of severe pain in the shoulder and arm with weakness in shoulder and biceps muscles for several weeks after a viral infection, but those with AIN syndrome do not. In a neuritis involving the AIN, spontaneous recovery usually occurs, although sometimes up to 1 year may be needed. In patients with a spontaneous AIN palsy and no electrodiagnostic evidence of reinnervation after 6 months, surgeons should consider nerve exploration or nerve transfer (or both). In patients with concomitant nerve compression, local decompression in patients with Parsonage-Turner syndrome may accelerate recovery.
Treatment
Because AIN palsy has a high rate of spontaneous recovery, except in rare cases of trauma or mass causing nerve dysfunction, patients should always be observed for several months before planning any surgical decompression.
In the absence of evidence suggesting neuritis, a trial of conservative management should always be given for at least 12 weeks before surgery. Surgical management is considered in patients who have a space-occupying mass in the area or in those who have failed to detect any clinical and electrodiagnostic signs of recovery approximately 6 to 12 months after starting nonsurgical treatment.
The surgical approach and decompression technique for the AIN in the forearm is the same as for pronator syndrome. All potential compressive sites should be released: the bicipital aponeurosis, the tendinous arch of the deep head of the pronator teres, any other tendinous bands (Gantzer accessory FPL muscle), and collateral vessels overlying the median nerve or the AIN. If no discrete pathology is demonstrated, the authors perform an epineurotomy of the median nerve in the elbow region and distal arm to look for intraepineurial constriction of nerve fascicles. Tendon transfers (or nerve transfer) can be performed 3 months later when there has been no neurologic recovery after release.
Ulrich and colleagues analyzed 14 patients with an AIN syndrome and performed surgical decompression if there were no signs of spontaneous recovery after 12 weeks of conservative treatment. Alexandre and colleagues reported 4 cases of pseudo-AIN neuropathies among 9 patients diagnosed as having AIN syndrome. They concluded that surgical exploration is indicated when EMG suggests a severe lesion, localized at a specific site of entrapment.
Ulnar nerve compression at the elbow: cubital tunnel syndrome
The ulnar nerve travels in the upper arm posterior to the medial intermuscular septum, anterior to the medial head of the triceps, piercing the intermuscular septum at approximately 5 to 10 cm above the elbow to enter the posterior compartment medially. The arcade of Struthers is a fibrous band running from the medial head of the triceps to the medial intermuscular septum. This fascial band crosses the ulnar nerve approximately 8 cm proximal to the medial epicondyle. The arcade of Struthers is present in 70% of patients and is a potential site of compression.
The ulnar nerve then travels posterior to the medial epicondyle through the cubital tunnel at the elbow. The roof of the cubital tunnel is defined by the arcuate ligament of Osborne. The Osborne ligament is a thickened fascia between the ulnar and humeral heads of the flexor carpi ulnaris (FCU). The floor of the cubital tunnel is formed by the medial collateral ligament of the elbow, the elbow joint capsule, and the olecranon. The nerve enters the forearm between the 2 heads of the FCU and continues deep along the FDP. The first branch off the ulnar nerve in most patients is a sensory branch to the elbow joint. The next branch is a motor branch to the FCU. Posterior branches of the medial antebrachial cutaneous nerve cross distal to the medial epicondyle at an average distal distance of 3.1 cm from the medial epicondyle (100%) and cross approximately 1.8 cm proximal to the medial epicondyle (61%). These cutaneous branches can be injured during cubital tunnel surgery. After ulnar nerve surgery, one of the most common causes of pain is the injury of the posterior branch of the medial antebrachial cutaneous nerve.
Cubital tunnel syndrome is the second most common compression neuropathy in the upper extremity. Fifty-two cases accounted for 28.5% of the authors’ cases of entrapment neuropathy in the upper extremity (see Table 1 ). It is the most common site of compression to the ulnar nerve between its origin at the brachial plexus and its site of entering the Guyon canal at the wrist. The ulnar nerve may be compressed at multiple levels.
Diagnosis: Cubital Tunnel
In the early phases of the disease, patients complain of medial elbow pain and paresthesias or numbness in the small finger and ulnar aspect of the ring finger. The disease later evolves to intrinsic muscle weakness and later atrophy. Patients notice weakness with grip and/or pinch strength or hand clumsiness. Increasing degrees of elbow flexion are provocative, in that they cause dynamic changes to the cross-sectional area and volume, affecting intra- and extraneural pressures. Longstanding disease can lead to irreversible intrinsic muscle atrophy. The extent of ulnar nerve dysfunction is divided into 3 categories by McGowan and modified by Dellon : (1) mild nerve dysfunction implies intermittent paresthesias and subjective weakness; (2) moderate dysfunction presents with intermittent paresthesias and measurable weakness; and (3) severe dysfunction is characterized by persistent paresthesias and measurable weakness.
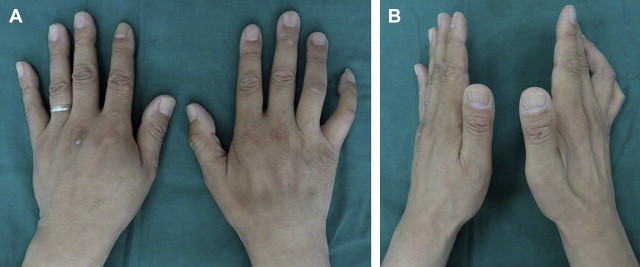
Clawing of the small and ring fingers is found in advanced stages ( Fig. 5 ). Atrophy of the intrinsic muscles of the hand and, in particular, the first dorsal interosseous muscle is common (see Fig. 5 ). The carrying angle may give a clue as to tracing back to prior trauma that increases the carrying angle and causes excess traction on the ulnar nerve. Careful sensory testing, such as touch 2PD testing, can help quantify early changes in sensibility. In the early stages of nerve compression, provocative testing (Tinel sign and elbow flexion-compression test) may be the only positive signs, followed by alteration of threshold testing (vibration and Semmes-Weinstein monofilaments). In the later stages, 2PD becomes abnormal. Motor strength should be assessed in all of the major upper extremity muscle groups, with particular attention paid to the intrinsic muscles of the hand and the deep flexors of the ring and small fingers.
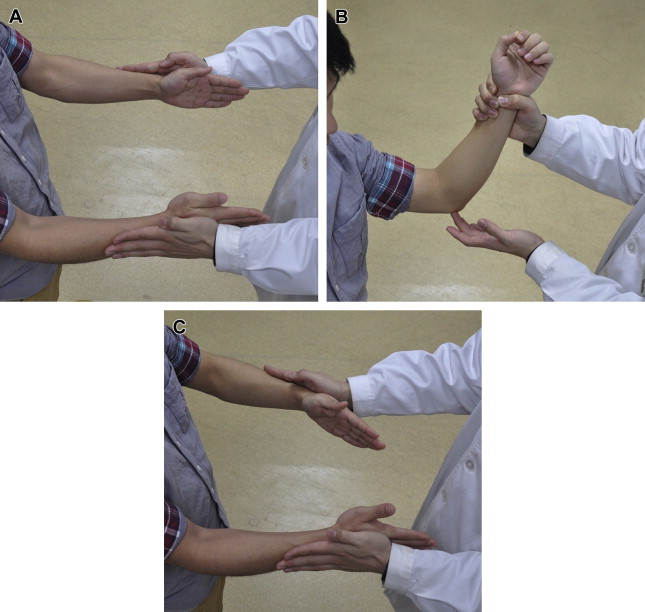
Two of the most frequently used provocative tests are the Tinel test along the course of the ulnar nerve and the elbow flexion-compression test. In 2008, Cheng and colleagues described the scratch collapse test ( Fig. 6 ). Sensitivity for this test was reported to be 69% compared with 54% and 46% for the Tinel test and the elbow flexion-compression test, respectively. The Tinel test, however, has the highest negative predictive value (98%) among all tests for cubital tunnel syndrome. These examination findings can be used in combination to best diagnose cubital tunnel syndrome.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


