Laser and energy-based devices interact with the skin in distinct ways. Not all interactions are created equal, and using improper settings can result in subtherapeutic, or worse, adverse outcomes. Understanding laser-tissue interactions is imperative for identifying and attaining appropriate, therapeutic endpoints. Energy-based devices that are not acting via selective photothermolysis will result in indicators that harken treatment outcomes. Warning endpoints and indicators communicate skin injury, and should promptly result in adjustment of treatment parameters.
Key points
- •
Laser and energy based devices communicate device-tissue interactions via signs on the skin termed endpoints and indicators.
- •
Therapeutic endpoints are indicative of a successful treatment, and suggest that a treatment will be effective. Warning endpoints are signs that point toward skin damage or undesired outcomes.
- •
Rather than using a cookbook approach, treatment settings should be tailored until therapeutic endpoints are achieved, and warning endpoints are avoided.
Introduction
When treating patients with lasers and light-based devices, distinct signs on the skin relay important messages to the device operator. It is imperative to watch for and understand these signs, first and foremost for patient safety. Warning signs should prompt the practitioner to discontinue treatment until appropriate setting adjustments have been made. Similarly, subtherapeutic signs should result in setting adjustments until there is a therapeutic result, or endpoint . The term endpoints refers most specifically to devices that harness the theory of selective photothermolysis and reflect laser-chromophore-tissue interactions. The term indicators refers to the laser-tissue interactions of other light-based devices.
This article will briefly provide an overview of laser-tissue interactions, as well as a review of both therapeutic and warning endpoints. Understanding and application of these concepts is imperative for success when using laser and light-based devices. While it can be easy to follow templates or suggested settings, these should serve only as starting points, and treatment parameters should ultimately be adjusted until appropriate endpoints are obtained. As a result, patients will benefit from successful, selective treatments, and will be spared from deleterious side effects.
Laser-tissue interactions
Understanding the principles of laser-tissue interactions is the first step to understanding endpoints. Laser light interacts with different components, called chromophores , in the skin (epidermis or dermis). The primary chromophores relevant to dermatology include water, hemoglobin, and pigment, including melanin. Chromophores absorb wavelengths of light in varying degrees, and the higher the selective absorption, the better a wavelength is suited for a chromophore. When a highly absorbed wavelength is beamed at a chromophore in the skin, the result is heating and/or destruction of the chromophore. The principle of selective photothermolysis, or The Anderson Principle, describes something of a Goldilocks phenomenon: if the light energy absorbed is just enough to destroy the target chromophore, surrounding tissues will be spared and left intact. Therefore, 2 additional components are key to laser-tissue interactions: the pulse duration , or time the chromophore is exposed to the laser light, and the fluence , or energy delivered per unit area.
When considering the appropriate laser modality and treatment settings, the chromophore directs the wavelength, and the size of the chromophore directs the pulse duration. Smaller targets (ie melanosomes) require very short pulse durations to selectively absorb laser energy, while larger targets (ie blood vessels) require longer pulse durations for adequate destruction and therapeutic effect. In general, the fluence should be titrated based on tissue endpoints, within limits. If an endpoint is not achieved despite appropriate setting adjustments, the laser operator must ask if there is another explanation. For example, an anemic patient may never respond to a pulsed dye laser (595 nm), despite hemoglobin’s selective absorption at this wavelength, as anemia results in low hemoglobin, and therefore inadequate chromophore.
Therapeutic endpoints
When extrapolating laser-tissue interactions to clinical settings, these fundamental principles correlate to treatment settings. This section will describe specific clinical conditions and the appropriate skin endpoints for therapeutic efficacy. The following section will provide warning and catastrophic endpoints, which should be avoided by starting low and going slow.
Vascular Lesions
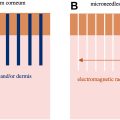
Vascular lesions are treated by targeting the chromophore hemoglobin. Based on the absorption spectrum of hemoglobin ( Fig. 1 ) [ ], this is best targeted with the commercially available 595 nm pulsed dye laser (PDL) or 532 nm potassium titanyl phosphate (KTP) laser. It is important to note that the absorption curve of oxyhemoglobin differs from that of deoxyhemoglobin, which has a unique absorption peak at around 755 nm. Consequently, venous lesions can be effectively and selectively treated at 755 nm, using an Alexandrite laser.
Port wine birthmarks
Port wine birthmarks (PWBs), also known as port wine stains (PWSs), are vascular birthmarks caused by endothelial cell proliferation resulting in ectatic, venous venule-like structures [ ]. While they typically start as flat lesions, they often become larger and can develop vascular outpouchings, termed blebs, over time. PWBs typically result from sporadic genetic mutations but can present as part of Sturge-Weber Syndrome, or other genetic syndromes.
Treatment of PWBs should begin early, while the lesions are as flat as possible. They typically recur and require maintenance over time. When treating PWBs, the appropriate endpoint is purpura ( Fig. 2 ). Notably, PWB in newborns may not have this endpoint. We typically use the 595 nm PDL (7–10 mm spot size) with short (0.45–3 msec) pulse durations at moderate to high fluences (4–9 J/cm2) to achieve this endpoint. As treatments progress and the chromophore becomes less dense, we often resultantly increase the fluence with treatments. The 532 nm KTP laser [ ] is also an appropriate and effective choice.

Care should be taken when treating heterogenous lesions as areas saturated with more chromophore may result in bulk heating and skin injury. Settings may need to be titrated across a lesion based on clinical findings of deeper red or purple-blue hues within the lesion. Additionally, nonresponsive PWBs, or those more blue-purple in color, can be treated with the 755 nm Alexandrite laser. The long pulsed 755 nm laser has a narrow therapeutic window. It is good practice to pick the darkest area of the birthmark and treat at, but not above, the fluence that achieves purpura. Distinct blebs in PWBs should be treated with care due to chromophore density.
Infantile hemangiomas
In the past, infantile hemangioma treatment was limited, and lasers were especially useful. However, new treatment modalities, including topical timolol and oral propranolol [ ], are highly safe and effective for treatment of infantile hemangiomas. As such, the use of lasers has declined over the years. Still, lasers are useful in combination with medical therapy or for treatment of hemangiomas resistant to medical therapy.
Infantile hemangiomas are dense in chromophore and can be susceptible to bulk overheating. Therefore, the desired immediate endpoint should be subtle, light, or even transient purpura. Frank purpura should prompt a decrease in fluence. Transient or very subtle purpura should be monitored as darkening of the lesion may occur post-treatment.
Telangiectasias
Telangiectasias are a common concern of patients and are typically responsive to PDL or KTP laser treatment. Perinasal telangiectasias can be refractory and typically require multiple treatments, with high recurrence rates. However, with appropriate counseling, treatment of telangiectasias can be very rewarding for clinician and patient. Immediate vessel darkening can be a therapeutic endpoint, but immediate vessel clearance is the preferred endpoint. We typically accomplish this using a 595 nm laser (3×10 or 7 mm spot size) with pulse durations ranging from 10 to 40 msec, depending on the size of the target vessel, with fluences ranging from 8 to 15 J/cm2. With increases in spot size, we typically decrease the fluence.
Cherry angiomas
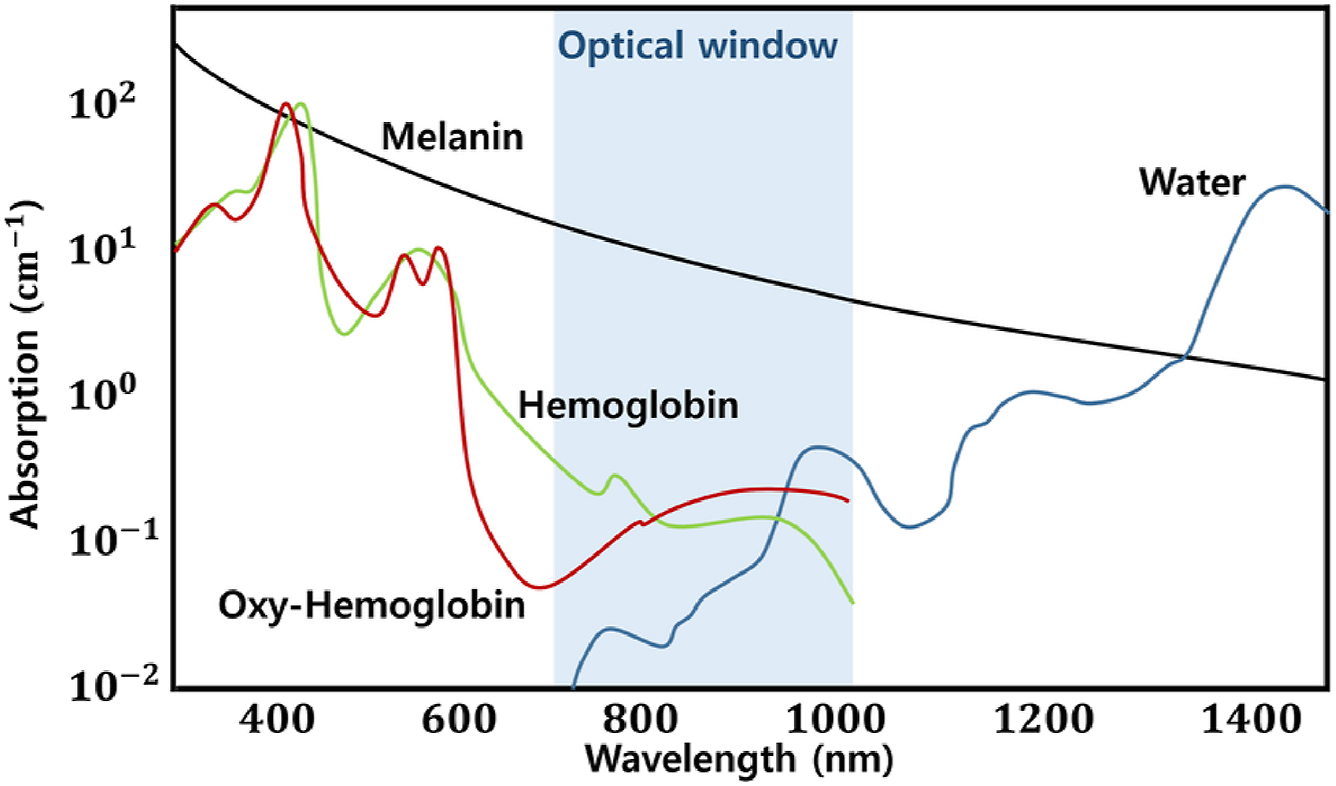
Small, flat cherry angiomas respond best to 595 nm or 532 nm laser light. The ideal endpoint is immediate purpura, without petechiae ( Fig. 3 A–C ). This typically indicates that the lesion will clear or lighten. We accomplish this with small spot sizes (3 mm) and short pulse durations (0.45–1.5 msec). Thick or large lesions may take multiple treatments. When using 595 nm or 532 nm light, if the ideal endpoint is not achieved with the first pulse, additional pulses may be fired after adequate skin cooling (typically 30 seconds–1 minute). Multiple lesions can be treated in one session, and any inadequately treated lesions can be retreated at the end of the session. When using 1064 nm laser light, pulse stacking should not be performed.
The technique of applying a glass slide to flatten the lesion, thereby increasing your chance of targeting a larger portion of the lesion, can be useful. However, care should be taken as the glass slide prevents epidermal cooling by cryogen cooling spray and cannot be used with ultrasound gel. Another technique we recommend is gentle outward stretching of the nearby skin, which can make the lesion flatter for the pulse.
Angiokeratomas can also be treated with the pulsed dye or KTP laser, including scrotal and labial angiokeratomas. A small spot size, short pulse duration, and moderately high fluence is generally required to achieve the therapeutic endpoint of purpura. Cooling should be high, and you can consider icing before and after treatment for comfort. The patient should be made aware that areas such as the scrotum and labia are prone to pigmentary changes.
Venous malformations
In addition to hemoglobin-rich vascular lesions, patients also present with deoxyhemoglobin-rich venous lesions. Large, soft, or disfiguring venous malformations should be treated surgically. However, some venous lesions, such as periorbital veins, spider veins, and venous lakes can be successfully treated with lasers. Typically, these vessels are larger, and therefore require longer pulse durations. Preferred wavelengths include 755 nm and 1064 nm. We treat periorbital veins using 1064 nm light, with a therapeutic endpoint of visible darkening or immediate disappearance of the vessel. We use small spot sizes (3–5 mm), and march along the vessel with longer pulse durations (20–50 msec) and relatively high fluences.
Pulse stacking should not be performed when using this wavelength (1064 nm)
Care should be taken to avoid overlap of pulses because of methemoglobin production from the laser pulse. The absorption of methemoglobin at 1064 nm is high, and overlap can result in ulcerations. When treating periorbital veins, caution should be used around the eye due to the depth of this wavelength.
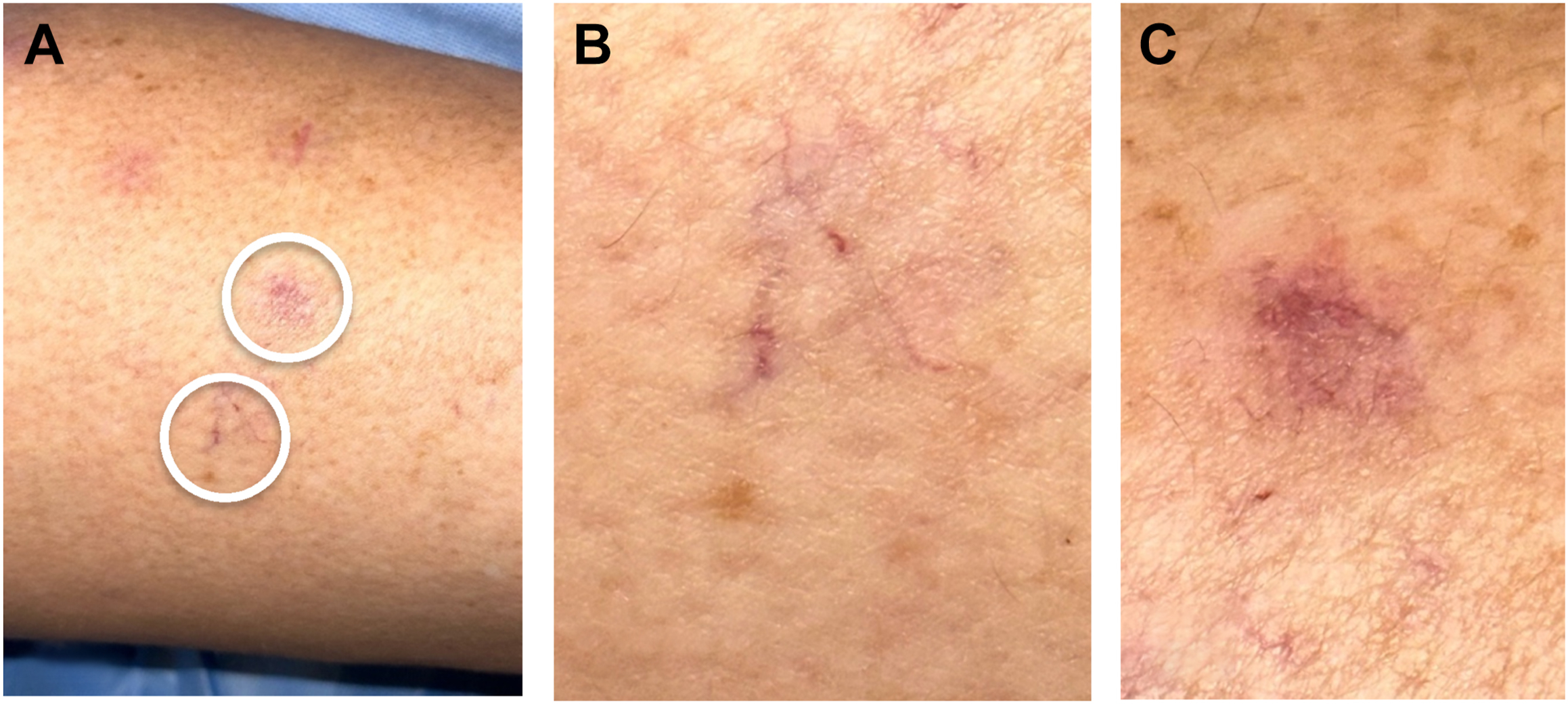
Other venous lesions, such as cutaneous leg veins or spider veins, can also be treated with lasers. Patient selection is important as large or tortuous vessels may require sclerosing therapy or surgical interventions. Small (<3 mm) blue vessels can be targeted with 1064 nm laser light using moderately long pulse durations (10–40 msec). The ideal endpoint is immediate disappearance or graying of the vessel. Small red and purple vessels on the legs respond well to the pulsed dye laser or KTP laser, similar to telangiectasias on the face (Image 3). Delayed endpoints (2–5 minutes) include a cat scratch or wheal-like appearance, and slightly purpuric areas of hemorrhage can be seen ( Fig. 4 A–C ).